")
Global maternity billing refers to the bundled reimbursement for routine pregnancy care, covering prenatal (antepartum), delivery, and postpartum services. These services are typically reported using a single CPT code, such as 59400 or 59510. These “global” codes streamline maternity billing but come with strict CMS rules that define what is and isn’t included in the package.
To avoid denied claims, OB/GYN billing teams must stay current with CMS guidelines, payer-specific policies, and recent updates that affect bundled care. This blog breaks down the 2026 CMS global maternity rules, highlights key coding scenarios, clarifies when unbundling is allowed, and shares strategies to ensure documentation compliance.
What “Global Maternity” Means Under Federal Policy?
Under federal policy, “Global Maternity” refers to the bundled payment structure defined by the Centers for Medicare & Medicaid Services (CMS) for routine obstetric care. It combines antepartum visits, delivery services, and postpartum care into one comprehensive reimbursement, rather than billing each service separately.
The global obstetrical package is reported with CPT 59400 for vaginal delivery or 59510 for cesarean delivery when one provider performs all components of care. Routine prenatal exams, labor management, delivery, and standard postpartum visits are included. However, ultrasounds, laboratory tests, and unrelated medical services are excluded and may be billed separately with proper documentation.
What are the Components Of The Global Obstetric Package?
The Global Obstetric Package refers to a bundled set of services covering the routine care a pregnant person receives from early pregnancy through delivery and into the postpartum period. It is widely defined in coding and obstetric practice guidelines (e.g., AMA CPT® and payer policies).
The global obstetric package comprises three core phases of maternity care:
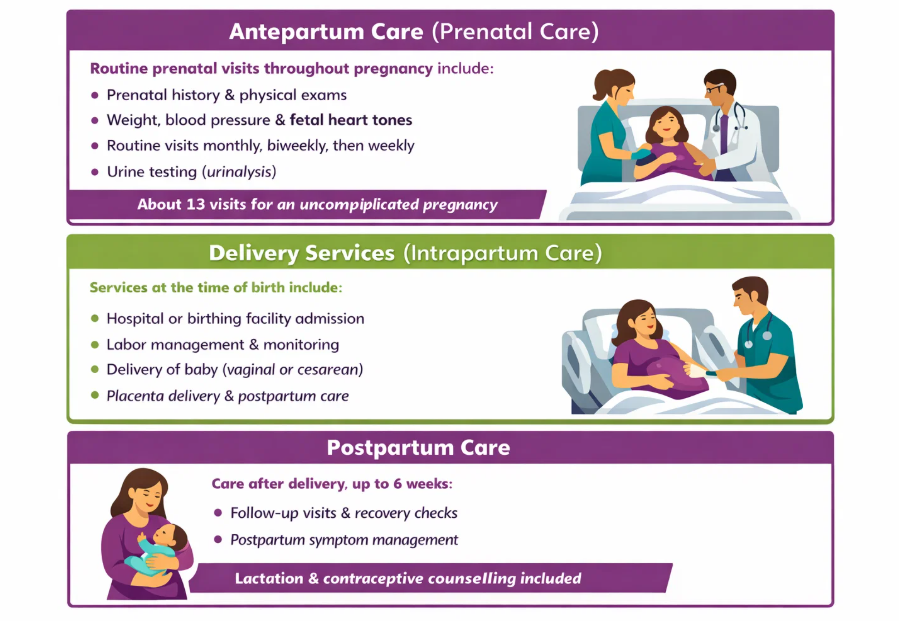
- Antepartum Care (Prenatal Care)
This includes routine, scheduled prenatal visits throughout pregnancy. Typical elements include:
- Prenatal history and physical examinations
- Recording weight, blood pressure, and fetal heart tones
- Routine visits spaced monthly, then biweekly, then weekly as pregnancy progresses
- Routine urine testing (urinalysis)
These routine visits usually total about 13 for an uncomplicated pregnancy.
- Delivery Services (Intrapartum Care)
Services provided at the time of birth, including:
- Admission to a hospital or birthing facility
- Labor management and monitoring
- Delivery of the baby (vaginal or cesarean)
- Delivery of placenta and immediate postpartum management
These are the core delivery-related professional services included in the package.
- Postpartum Care
Routine care provided after delivery, typically up to about 6 weeks, including:
- Follow-up visits to assess recovery and general health
- Management of uncomplicated postpartum symptoms
This supports the patient’s recovery after birth and can include lactation and contraceptive counseling as part of routine care
How Global Obstetric Package is Used in Billing?
In medical coding, these services are not billed separately when provided by the same clinician or practice group. On the other hand, they are reported under a global obstetric code (e.g., CPT codes 59400, 59510, 59610, 59618 depending on delivery type).
What Is Generally Not Included?
Certain services that may occur during pregnancy are not part of the global package and are billed separately, such as:
- Ultrasound imaging
- High-risk or complication-driven visits
- Laboratory tests beyond routine urinalysis
- Procedures such as amniocentesis or non-stress tests
- Care unrelated to pregnancy
These exceptions help differentiate routine bundled care from additional services requiring separate codes.
What Is The Typical Global Period And Coverage Window?
Most payers follow the six-week postpartum rule, meaning the global package includes one routine post-delivery visit, usually performed around six weeks after birth. For example, BlueCross BlueShield of Vermont states that CPT 59430 covers postpartum care visits provided within six weeks following delivery.
Although CMS assigns a 90-day global period, the practical postpartum care window for routine services generally extends to about 42 days after delivery. After this timeframe, any additional postpartum visits or treatment for complications must be billed separately using appropriate evaluation and management codes.
Centers for Medicare & Medicaid Services does not reimburse services beyond routine postpartum care under the global code unless a separate medical necessity is properly documented. If a patient presents with an unrelated medical problem during the 90-day global period, providers must report the visit with modifier -24 to indicate a distinct service.
CMS Policy and Coding Requirements Specific to Global Maternity
A clear understanding of CMS rules is essential for compliant obstetric billing. Below are the core Medicare policy and coding requirements that directly affect global maternity claims.
Medicare Global Period Designation (MMM) and How It Applies
Medicare marks obstetric package codes with the “MMM” global period to distinguish them from standard surgical global periods. Thus, a code like 59400 or 59510 carries the MMM designation, bundling prenatal care, delivery, and the postpartum visit into one payment. As CMS guidance states, these bundles are treated like major surgeries for purposes of global rules.
In practice, this means pre- and post-delivery visits are not billed separately (they are considered part of the package), except under rare circumstances where CMS/NCCI allows distinct coding. MedCare billing experts emphasize that Medicare’s MMM policy “distinguishes” obstetric codes from other global periods, yet otherwise applies standard global-surgery rules to them.
Required Documentation and Claim Submission Standards for Global Obstetric Package
Detailed medical records are required to support any global OB claim. Charting should clearly document prenatal history, patient dates of service, fetal status, complications, and delivery details. For example, Blue Cross notes that obstetric documentation should specify gestational age at each visit, whether the pregnancy is first or subsequent, the number of fetuses, and any high-risk conditions. Payers may specifically require listing the number of prenatal visits on the claim.
California’s Medi-Cal policy mandates that providers using global billing render 8–13 antepartum visits and document them in claim remarks. If fewer than 8 visits occur, the provider must bill for each visit instead. Likewise, global OB claims typically must be submitted in a “from–through” date format. This ensures the claim spans the entire pregnancy window.
Another example: a pregnancy confirmation visit before initiating prenatal care should be billed separately and is often reported with a Category II code. In all cases, plans insist that all codes on the claim be fully supported by the medical record. Submission of any OB code without documentation matching the service can trigger a denial.
Timely Filing and Reimbursement Compliance
All global maternity claims are subject to standard timely-filing limits. In practice, this means claims must generally be sent within 12 months from the date of service. Medicaid and commercial payers often follow similar deadlines. If a global claim is late, it is usually not payable except in very rare cases.
Beyond filing deadlines, compliance also means avoiding coding mistakes that could affect reimbursement. Insurers are increasingly auditing obstetric claims after payment, so incorrect coding or missing documentation often leads to denials even after an initial payment.
Thus, practices must track deadlines and maintain audit-ready records. Internal audits or claim edits should catch errors early. In short, adhering to both CMS global policy and each payer’s submission rules is essential to secure full payment and avoid recoupments.
Partial Global, Component, and Split Billing Scenarios
Global maternity billing does not apply when a provider furnishes only part of the pregnancy care. The following are the key scenarios where partial, component, or split billing rules apply:
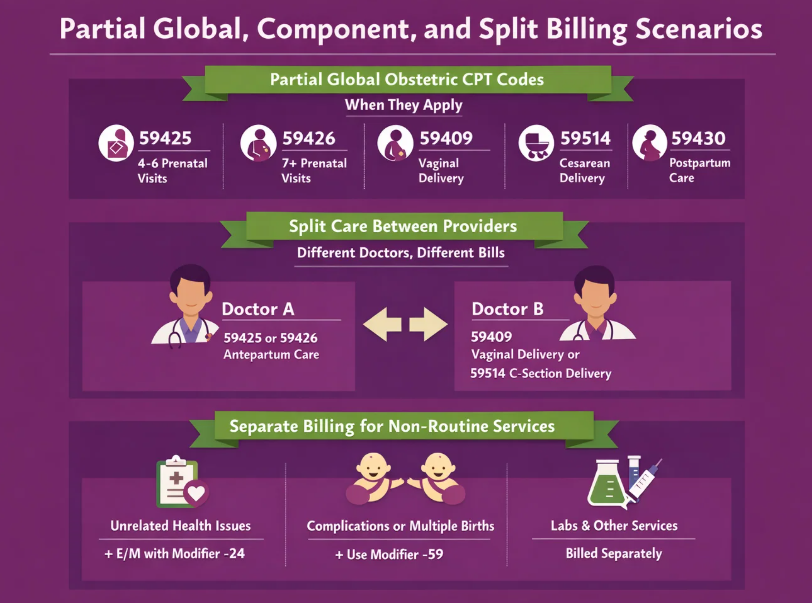
Partial Global Obstetric CPT Codes and When They Apply
The component (partial) codes for obstetrics cover specific segments of maternity care. Antepartum-only codes include 59425 for 4–6 visits and 59426 for 7 or more, while 59409 covers vaginal delivery, 59514 covers cesarean delivery, and 59430 is for postpartum care.
These codes are used when your practice provides only part of the maternity care (for example, only prenatal visits or only the delivery). The MedCare OB billing guide lists these codes explicitly. A provider’s choice of code must match the services delivered.
For instance, if a doctor saw the patient 5 times antepartum and then referred her elsewhere for delivery and postpartum, that doctor should bill 59425 (antepartum-only). Likewise, 59430 (postpartum-only) exists to cover the situation where one physician provides routine postpartum care but did not do the delivery.
Split Care Between Providers
In split-care scenarios, payer policies clarify who can bill a global code. For example, if one physician/group handles antepartum (and perhaps postpartum) and another unaffiliated physician does the delivery, neither may use the global package.
Each bills separately for its portion. In that case, the first doctor bills antepartum (using 59425/59426) and the second bills delivery only (e.g., 59409 or 59514). However, if two doctors are in the same practice group, a global code may be used by one provider for the entire bundle.
Separate Billing for Services Outside the Package
Services outside the routine global package must be billed separately. Routine prenatal procedures (like standard screening ultrasounds) are usually considered part of the global fee. For example, ultrasounds performed as routine prenatal screening are bundled into the OB fee. By contrast, any service unrelated to the pregnancy should be coded independently.
Non-pregnancy issues encountered during pregnancy should be documented and billed as an E/M for a separate problem, with modifier 24 and the unrelated condition as the primary diagnosis. Similarly, surgical complications may be billed separately. In multiple births, the CPT definition allows billing a second delivery using modifier 59.
Services like office supplies, vaccines, or lab tests unrelated to routine OB are also payable separately. In sum, anything beyond the AMA-defined antepartum/delivery/postpartum continuum, documented as distinct or unrelated, must be coded and billed outside the global package.
CMS Exceptions and Payer Variations
Although CMS establishes the foundational framework for global maternity billing, reimbursement policies can vary across Medicare, Medicaid, and commercial payers. Here are
Medicare vs Medicaid vs Commercial Payer Policies
Policies can vary by program and insurer. Medicare follows the MMM global rules nationwide, but its contractors (MACs) may publish guidance on billing details. State Medicaid programs often mirror Medicare’s code set but can have special rules.
For instance, one state policy noted that global maternity codes are accepted only when Medicaid is the secondary payer (they deny the global package when Medicaid is primary). Others may require “split” obstetrical rules or enforce specific claim edits.
By contrast, commercial insurers usually align with CMS and CPT guidance for global OB, but individual carriers can impose their own limits. Many commercial plans follow Medicare’s lead; they may differ in exact inclusions, such as how many postpartum visits are bundled or what telehealth services are covered.
When CMS Allows Exceptions?
Regarding CMS exceptions, strict bundling rules generally apply. Medicare rarely makes special allowances beyond those in the CPT manuals and NCCI edits. Separate payment is only allowed when services clearly fall outside the global package by policy.
For example, an E/M visit with modifier 25 on the delivery day for a significant separate condition, or a truly unrelated postpartum problem coded with modifier 24. CMS does not allow exceptions to global obstetric billing rules unless a specific code or modifier is clearly permitted by the payer’s policy.
Documentation and Coding Best Practices for Compliance
To ensure compliance and get full reimbursements from insurers, practices must follow these documentation and coding best practices.
Clinical Records That Support Global Billing
Maintain comprehensive obstetric records detailing every prenatal, delivery, and postpartum encounter. Each entry should note gestational age, visit date, purpose, and any high-risk conditions. Delivery notes must record labor details, type of delivery, any lacerations or interventions, fetal outcomes, and location of delivery.
Likewise, postpartum visit notes should capture the 4–6 week check (vital signs, any wound checks, and OBGYN exam findings). All entries should align with ICD-10 diagnoses. Insurers may request the full OB record when reviewing a global claim, so ensure each billed code is clearly matched by documentation.
CPT Code Selection Accuracy
Use the CPT code that exactly reflects the care provided. Only bill a global maternity code if your practice truly manages routine antepartum, all aspects of delivery, and routine postpartum care. According to Medicaid guidelines, if a provider performed four or more prenatal visits and handled both the delivery and postpartum, they must bill the global OB code.
If the circumstances differ, use the component codes. For example, bill 59425 or 59426 if you provided prenatal care only, or 59409/59514 for a delivery-only scenario, or 59430 if only postpartum care was given. When billing VBAC cases, select the correct code based on the services provided. Use 59610 for a full global VBAC package, and 59612 if only the VBAC delivery was performed.
Do not report antepartum E/M visit codes alongside the corresponding global or partial antepartum code, as that would double-count the same encounter. In summary, carefully count your visits and services against the CPT definitions.
Proper Use of Modifiers
Proper modifier application is critical for compliant global obstetric billing. The following are the key modifiers and their appropriate use in OB GYN claims processing.
| Modifier | When to Use | Key Documentation Requirement | Important Notes |
|---|---|---|---|
| 25 | Significant, separately identifiable E M service on the same day as a procedure or delivery | Record must show distinct medical decision making beyond routine obstetric care | Frequently misused on OB claims, documentation must clearly support a separate evaluation |
| 24 | Unrelated E M service during the postpartum global period | Diagnosis must reflect a condition unrelated to pregnancy or delivery | Append to E M code and report unrelated diagnosis as primary |
| 59 or X modifier | Second delivery procedure in multiple birth cases | Documentation must confirm distinct procedural service | Used to indicate a separate and independent delivery service |
| 80 | Assistant surgeon participation in cesarean delivery | Operative report must identify assistant role | Append to delivery only code such as 59514 |
| Do not use | Irrelevant modifiers such as 90 or 91 | Not applicable to global obstetric claims | Laboratory modifiers should never be appended to OB global billing |
Major Maternity/OB‑GYN Code Changes Coming in 2027
Here are the new and upcoming CPT coding changes related to maternity and OB/GYN billing based on the September 2025 CPT Editorial Panel actions. These will be effective January 1, 2027, which is a major update that practitioners must know:
1. New CPT Codes for Maternity Care Services (59XX1 – 59X12)
The Editorial Panel accepted new CPT codes numbered 59XX1 through 59X12 specifically to report maternity care services with updated coding guidelines. These are intended to replace a large portion of the current global obstetric code structure.
2. Deletions of Existing Global Maternity/OB Codes
Many traditional global obstetric codes will be deleted when the new codes take effect, including but not limited to:
- 59400 (global OB, vaginal delivery)
- 59409 (vaginal delivery only)
- 59410 (antepartum only)
- 59425/59426 (partial prenatal)
- 59430 (postpartum only)
- 59510 (global OB, cesarean)
- 59514 (cesarean delivery only)
- 59525, 59610, 59612, 59614, 59618, 59620, 59622 (OB/VBAC and related component codes)
3. Revisions to Related Codes and Guidelines
The panel also revised guidelines and descriptors for several existing codes that interact with maternity/OB care, such as 59412, 59051, 59300, 59898, and 59899. This signals a broad restructuring of how obstetric services are reported in CPT.
FAQS
How does Transcure help my practice with global maternity claims?
Transcure specializes in OB/GYN medical billing to ensure global maternity claims are accurately coded and submitted according to CMS and payer guidelines. They handle documentation review, modifier application, and claim follow-ups, maintaining 99.99% clean claim accuracy.
Which are the best OB/GYN billing companies in the United States?
The best OB/GYN billing companies in the U.S. include Transcure, Invensis, and BillingFreedom. However, Transcure stands as the top OB/GYN billing firm, which offers end-to-end billing support and is well-versed with the CMS global maternity guidelines. Moreover, its high performance metrics, including 99.99% clean claim accuracy, only 1% claim denial rate, and up to 20% revenue boost, make it a reliable company.
How are multiple births billed under global maternity rules?
Under global maternity rules, the first delivery is billed using the standard global OB code. On the other hand, a second or additional delivery can be reported separately using modifier 59 to indicate a distinct service. Each provider must document the separate deliveries clearly to ensure proper coding and reimbursement.
What is the timely filing limit for OB/GYN claims with major US insurers?
For most major U.S. insurers, including Medicare and commercial payers, OB/GYN claims must typically be submitted within 12 months from the date of service. Late claims are usually denied unless exceptional circumstances or payer-specific extensions apply.