
Podiatry billing has one of the worst improper payment rates in Medicare. According to CMS, podiatry care’s 2024 improper payment rate hit 11.2%. This means roughly $216.9 million was paid in error. Most of those errors don’t come from coding only.
Insufficient documentation drove 76.4% of improper payments, with incorrect coding at 11.5%, missing documentation at 7.2%, and medical necessity failures at 4.4%. In podiatry billing and coding, the break point is almost always documentation tied to routine foot care, class findings, and Q-modifier use.
Hence, knowing everything about podiatry billing is a must when it comes to getting the best podiatry billing services. This guide covers the podiatry billing workflow, Medicare coverage rules, modifier logic, and denial management.
Why Podiatry Billing Is Different from General Medical Billing
Podiatry medical billing uses the same CPT, ICD-10, and HCPCS code sets as the rest of healthcare. The rules around when those codes pay and when they don’t are what set this specialty apart.
What Podiatry Billing Covers
Podiatry billing covers diagnostic, surgical, and routine care for the foot, ankle, and lower extremity. That includes nail debridement, callus paring, wound care, fracture treatment, bunionectomies, hammertoe correction, orthotic fitting, and tendon repair. Each category carries its own coverage rules and modifier requirements.
How Podiatry Differs from Other Specialties at the Billing Level
Three structural factors make medical billing for podiatrists fundamentally different.
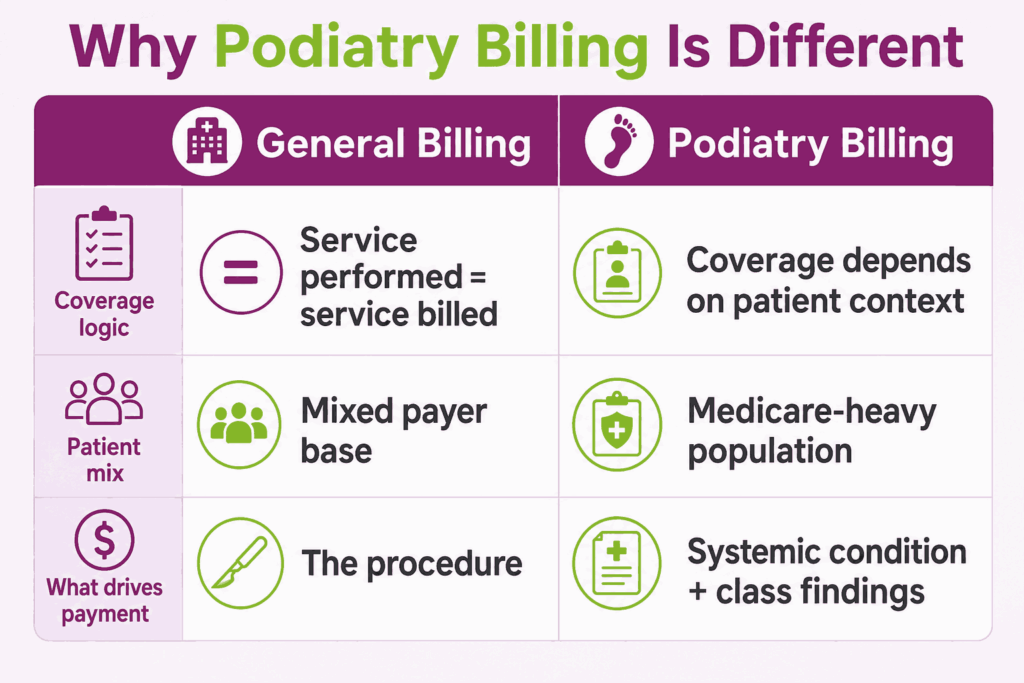
Routine vs. Medically Necessary Care
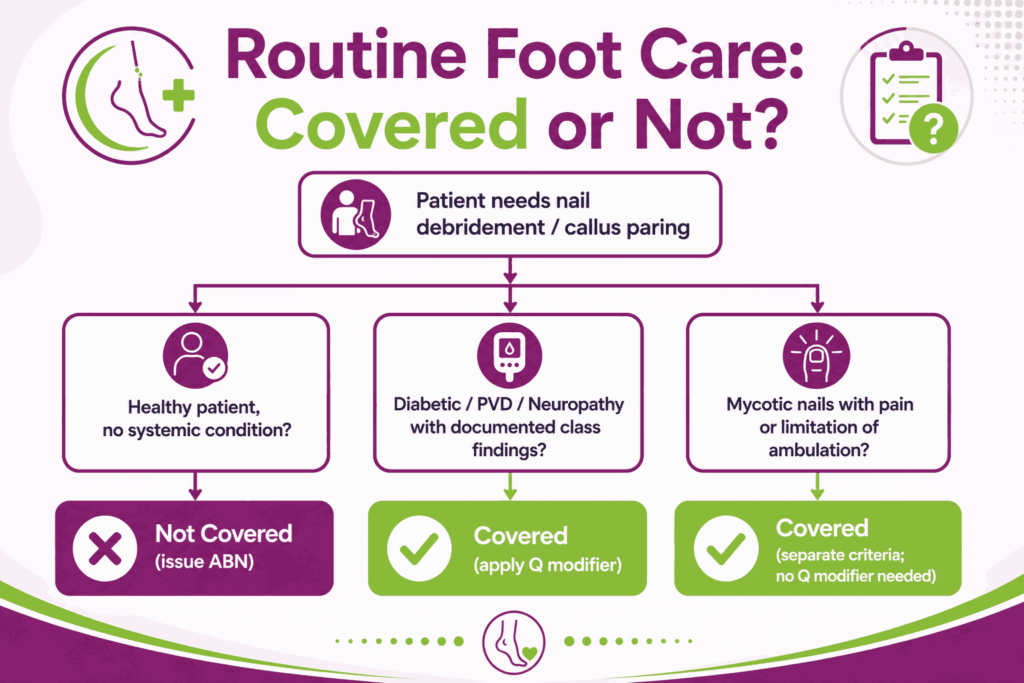
In most specialties, performing a service is enough to bill it. In podiatry, the same procedure can be covered or excluded based on why it was done. Trimming a toenail for a healthy patient is routine foot care, and Medicare doesn’t pay. Trimming the same toenail for a diabetic patient with documented neuropathy is medically necessary, and Medicare pays.
Heavy Medicare Patient Population
Podiatry serves one of the oldest patient populations in outpatient care. That puts Medicare podiatry billing rules at the center of every claim, including LCD compliance and frequency limits. Commercial payers usually mirror Medicare’s logic, so weak Medicare processes drag down commercial collections too.
Coverage Tied to Systemic Conditions, Not the Procedure
Routine foot care is covered only when paired with a qualifying systemic condition, such as diabetes, peripheral vascular disease, or peripheral neuropathy. This must also be supported by podiatry class findings like Class A, B, or C. The coverage depends on the patient, not the procedure.
Why These Differences Drive Higher Denial Rates
These dependencies stack. A single routine foot care claim needs the right diagnosis code, documented class findings, the correct Q modifier, and proof that the frequency limit hasn’t been exceeded. Miss any one, and the claim fails. No other specialty layers this many requirements on a single line item, which is why podiatry billing denials run higher than most outpatient specialties.
What Does the Podiatry Billing Workflow Include?
A consistent podiatry medical billing process turns coverage rules and modifier complexity into predictable revenue. The seven podiatry billing steps below run from intake to payment. Skip one, and the denial waits at the end.
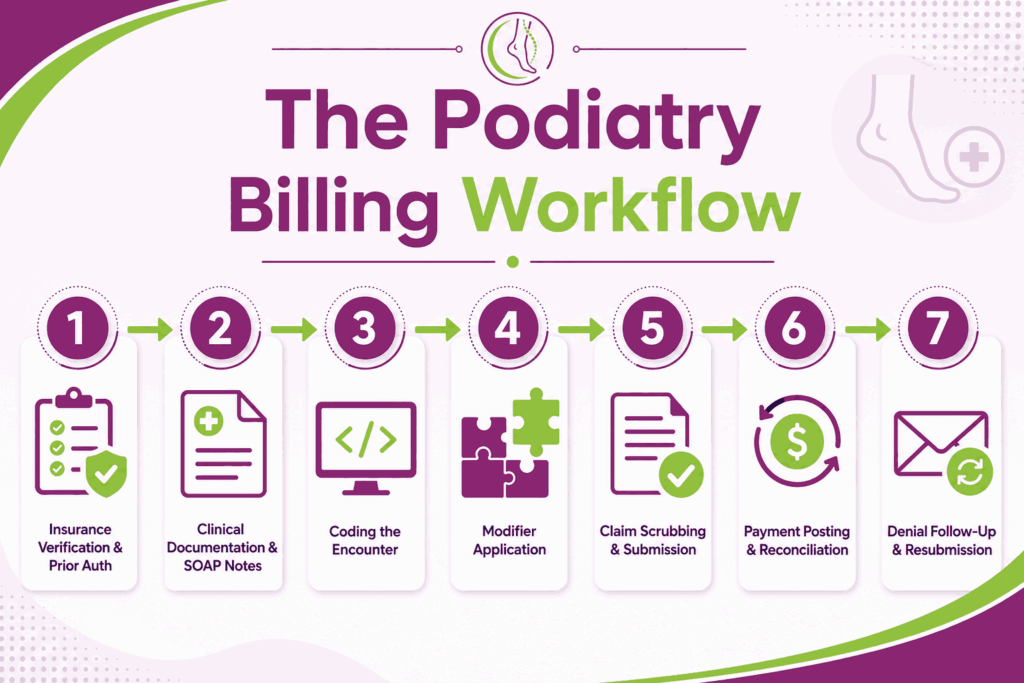
Step 1: Insurance Verification and Prior Authorization
Verification happens before the visit, not after.
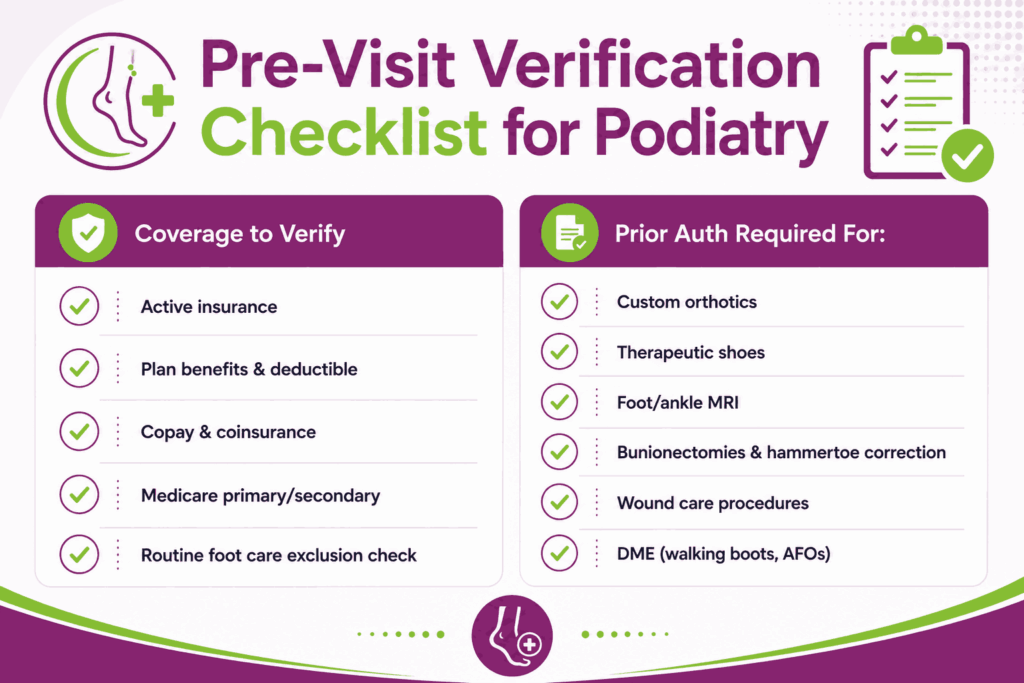
What to Verify Before the Visit
Confirm active coverage, plan benefits, deductible status, copay, and whether Medicare is primary or secondary. For podiatry, also check whether the payer treats foot care as a routine exclusion and which diagnosis codes trigger coverage. Document everything in the patient file.
Procedures That Typically Require Prior Auth
Custom orthotics, therapeutic shoes, MRI of the foot or ankle, most bunionectomies and hammertoe corrections, and selected wound care procedures usually need prior authorization. DME, like walking boots and AFOs, also fall here. Missing prior authorization in podiatry is one of the top three denial reasons in this specialty.
Step 2: Clinical Documentation and SOAP Notes
Every visit needs a complete podiatry SOAP note: Subjective, Objective, Assessment, Plan.
Documenting Medical Necessity
The note has to justify why the service was performed. Podiatry documentation requirements for routine foot care include the qualifying systemic condition, physical exam findings, the date the patient was last seen by the managing physician (required in some MAC jurisdictions), and the clinical reason a podiatrist had to perform the service.
Capturing Systemic Conditions and Class Findings in the Record
Document the systemic diagnosis and the specific class findings observed, such as absent pulses, trophic changes, claudication, and paresthesia. The class findings must be tied to the same foot being treated, not “both feet” or “lower extremities.” Because missing even one localized finding can cause an automated rejection, utilizing the top podiatry billing EMRs is critical for independent practices.
These specialty platforms build hard stops and intelligent compliance prompts directly into the SOAP note workflow, preventing providers from closing an encounter until all necessary class findings and data points are mapped.
Step 3: Coding the Encounter
Each claim must be coded accurately for every type of required coding category.
CPT, ICD-10, and HCPCS Basics
Each podiatry encounter codes across three sets: CPT for procedures, ICD-10 for diagnoses, and HCPCS Level II for supplies, orthotics, and DME. CPT covers nail debridement, wound care, injections, and surgeries. ICD-10 captures the systemic condition, laterality, and severity. HCPCS handles L-codes for orthotics and A-codes for therapeutic shoes. For a complete code list with examples, see our podiatry CPT codes cheat sheet.
Linking Diagnosis to Procedure (“No Diagnosis, No Dollars”)
Every procedure must be tied to a supporting diagnosis on the claim. An 11721 nail debridement without a qualifying systemic condition denies automatically. The diagnosis proves medical necessity; the procedure is what gets paid. No diagnosis, no dollars.
Step 4: Modifier Application
Modifiers tell the payer how to interpret the claim. For routine foot care, apply the Q modifier that matches the documented class findings. Q7 for one Class A finding, Q8 for two Class B findings, Q9 for one Class B plus two Class C findings. Add LT or RT for laterality, and TA or T1–T9 when a specific toe was treated.
Use modifier 25 when a separately identifiable E/M is performed on the same day as a procedure, and modifier 59 when two procedures need to be unbundled. Modifier errors drive a significant share of podiatry denials, which is why this step deserves a dedicated QA check before submission.
Step 5: Claim Scrubbing and Submission
Scrub every claim before it leaves your system.
NCCI Edit Checks
The CMS National Correct Coding Initiative (NCCI) flags mutually exclusive code pairs and unbundling errors. Most clearinghouses run NCCI edits automatically. When a bundle risk exists, weigh the higher-RVU code as primary.
Clearinghouse vs. Direct Payer Submission
Most practices route through a clearinghouse for batch scrubbing, eligibility checks, and rejection reports. Direct submission to the payer portal is faster for single claims but skips pre-submission validation. Use clearinghouses for volume; reserve direct submission for corrections and appeals.
Step 6: Payment Posting and Reconciliation
Post payments against the original claim, reconcile against the EOB or ERA, and flag any underpayments against your contracted fee schedule. Track adjustments by reason code to surface payer-specific patterns over time.
Step 7: Denial Follow-Up and Resubmission
Work denials daily, not weekly. Pull the denial reason code from the ERA, categorize the issue like missing information, coding error, no authorization, medical necessity, or frequency limit. Then, decide whether to correct and resubmit or file a formal appeal.
Track timely filing windows for each payer; most run 90 to 180 days, but some commercial payers cut tighter. Log every denial by reason code so you can fix the upstream process, not just the individual claim.
What Are Medicare Coverage Rules for Routine Foot Care
Medicare denies more podiatry claims for coverage issues than for coding errors. The Medicare podiatry guidelines below, such as routine foot care exclusion, systemic condition exceptions, class finding framework, and frequency rules, are what separate a clean claim from a denied one.
The Routine Foot Care Exclusion
Medicare classifies routine foot care as a statutory exclusion under the Medicare Benefit Policy Manual, Chapter 15, Section 290. The rule: cutting or removing corns and calluses, trimming and debridement of nails, and other hygienic foot care are not covered when performed on a patient without an underlying systemic condition. Coverage is the exception, not the default.
Four narrow paths to coverage exist: the service is integral to another covered service, treatment of warts on the foot, presence of a qualifying systemic condition with documented class findings, or treatment of mycotic nails meeting specific criteria.
Qualifying Systemic Conditions for Covered Foot Care
Medicare’s “presumption of coverage” applies when the patient has a systemic disease severe enough to make routine foot care hazardous if performed by anyone other than a qualified podiatrist.
Diabetes Mellitus
Diabetes (ICD-10 E08–E13) is the most common qualifying condition. The diagnosis alone isn’t enough, as documentation must show diabetic complications such as neuropathy, peripheral angiopathy, or foot ulceration. The date last seen by the managing physician (DLS) may also be required on the claim in some MAC jurisdictions.
Peripheral Vascular Disease
PVD (I73.9 and related codes), arteriosclerosis of the extremities (I70.2x), and chronic venous insufficiency (I87.2) all qualify. Documentation must show evidence of impaired circulation, such as diminished pulses, claudication, or vascular study results.
Peripheral Neuropathy
Sensory neuropathy from any cause, such as diabetic (E11.40x), idiopathic (G60.9), or drug-induced (G62.0), qualifies when loss of protective sensation (LOPS) is documented. Monofilament testing is the standard documentation method.
Class A, B, and C Findings Explained
Podiatry class findings are the physical exam observations Medicare requires alongside the systemic diagnosis to establish podiatry medical necessity. Findings must be documented on the same foot being treated.
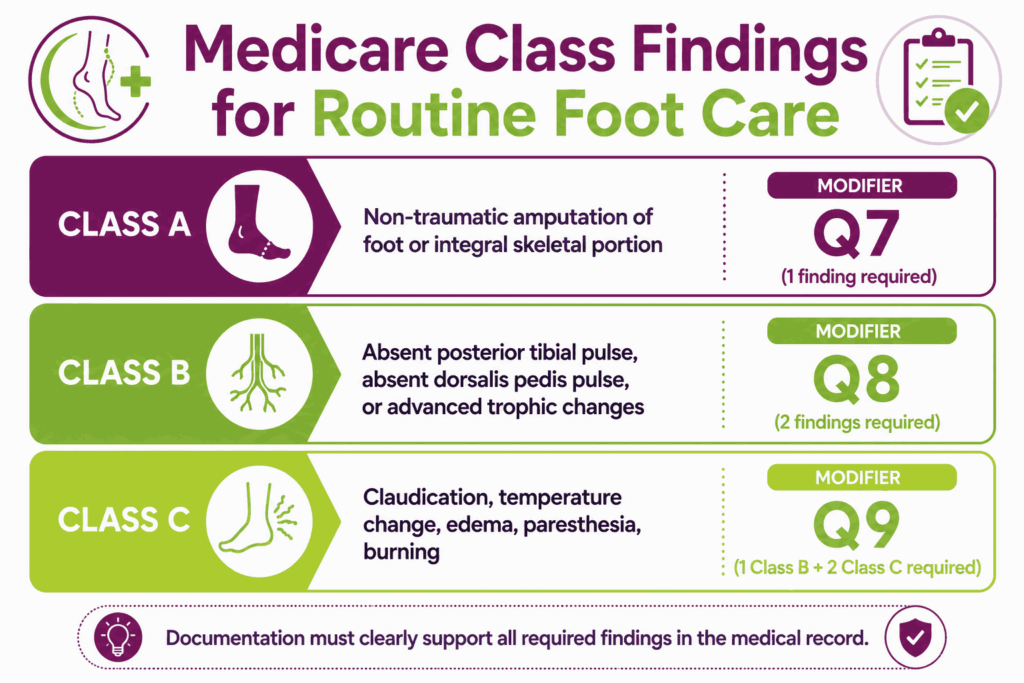
Class A Findings
Non-traumatic amputation of the foot or integral skeletal portion. One Class A finding alone supports coverage (paired with modifier Q7).
Class B Findings
Absent posterior tibial pulse, absent dorsalis pedis pulse, or advanced trophic changes (three of: decrease or absence of hair growth, nail thickening, pigmentary changes, thin shiny skin texture, rubor or redness). Two Class B findings support coverage (paired with modifier Q8).
Class C Findings
Claudication, temperature changes, edema, paresthesia, or burning. One Class B plus two Class C findings support coverage (paired with modifier Q9).
The 60-Day Frequency Rule for Routine Foot Care
Covered routine foot care is medically necessary once every 60 days. More frequent services may be paid only if documentation clearly justifies the clinical need and is supported by the managing physician’s notes. Services exceeding this frequency get flagged for medical review.
Mycotic Nail Debridement Coverage Criteria
When a systemic condition is absent, Medicare can still cover nail debridement (11720, 11721) if the patient has clinical evidence of mycosis plus one of two scenarios. An ambulatory patient with marked limitation of ambulation, pain, or secondary infection from the thickened nail, or a non-ambulatory patient with pain or secondary infection from the same. Both the mycosis diagnosis and the secondary symptom must be coded on the claim.
ABN: When and How to Use It
An Advance Beneficiary Notice of Noncoverage (CMS-R-131) lets the patient choose whether to receive a service Medicare is likely to deny. Use it whenever you reasonably expect a denial, like routine foot care without qualifying conditions, services exceeding frequency limits, or procedures lacking documented medical necessity.
Attach modifier GA when the ABN is on file, GY for statutorily excluded services, or GZ when you expect a denial, but no ABN was obtained. Without a valid ABN, you cannot bill the patient for a denied service.
What Are the Most Common Modifiers Used in Podiatry Billing?
Podiatry billing modifiers signal why and how a service was performed. Basically, the difference between a paid claim and a denial. They’re the second-largest source of podiatry billing denials after documentation failures.
Q7, Q8, Q9: Class Finding Modifiers
Q modifiers prove medical necessity for routine foot care under Medicare. They pair with CPT codes 11055–11057, 11719–11721, and G0127. Submit a routine foot care claim without a Q modifier on a patient with a systemic condition, and Medicare denies it automatically.
Modifier Q7: One Class A Finding
Use modifier Q7 in podiatry when the patient has one Class A finding: non-traumatic amputation of the foot or an integral skeletal portion. Document the level and side (e.g., transmetatarsal amputation, left foot).
Modifier Q8: Two Class B Findings
Use modifier Q8 in podiatry when two Class B findings are documented on the same foot. Any combination of absent posterior tibial pulse, absent dorsalis pedis pulse, or advanced trophic changes.
Modifier Q9: One Class B and Two Class C Findings
Use modifier Q9 in podiatry when one Class B finding pairs with two Class C findings on the same foot. Class C findings include claudication, temperature change, edema, paresthesia, or burning.
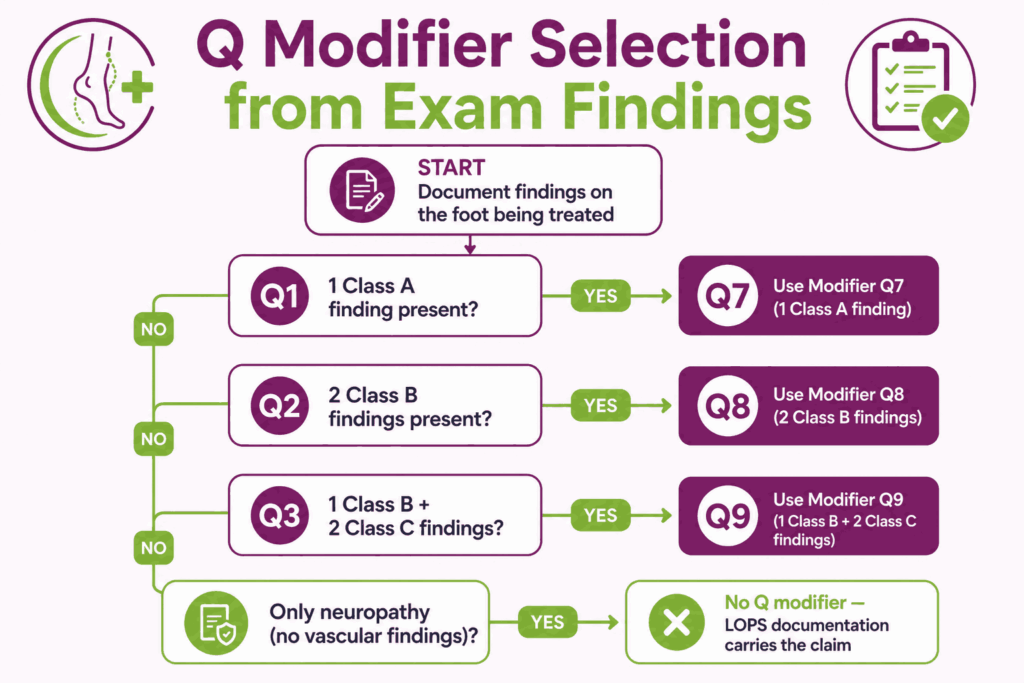
Decision Tree: Choosing the Right Q Modifier
Start with the exam findings on each foot, not “both feet.” One Class A finding → Q7. Two Class B findings → Q8. One Class B plus two Class C → Q9. If only peripheral neuropathy without vascular findings is documented, no Q modifier applies. The LOPS documentation carries the claim.
Modifier 25: Significant, Separately Identifiable E/M
Attach modifier 25 in podiatry billing when an E/M service is performed on the same day as a procedure and goes beyond the usual pre- and post-procedure assessment.
Example: 99213-25 paired with 11721 when a separate problem is evaluated during the nail debridement visit. HHS OIG audits routinely target modifier 25 misuse, so the supporting documentation must clearly justify the separate E/M.
Modifier 59: Distinct Procedural Service
Modifier 59 in podiatry unbundles two procedures that NCCI edits would normally pair. Use it only when no more specific modifier applies.
Example: 11055 (callus paring) on the right foot + 17110 (wart destruction)-59 on the left, separating two distinct services performed at different sites.
LT and RT: Laterality Modifiers
LT and RT modifiers in podiatry identify the side treated: LT for the left foot, RT for the right. Apply them to every podiatry procedure performed on a specific foot. Missing laterality is a common cause of duplicate-claim denials when the same procedure is billed for both feet on the same day.
TA and T1–T9: Toe-Specific Modifiers
T modifiers in podiatry identify the specific toe treated: TA = left great toe, T1–T4 = left second through fifth toes, T5 = right great toe, T6–T9 = right second through fifth toes. Required when the procedure is toe-specific (e.g., hammertoe correction, partial nail avulsion) and the payer needs to distinguish multiple toe procedures on the same date.
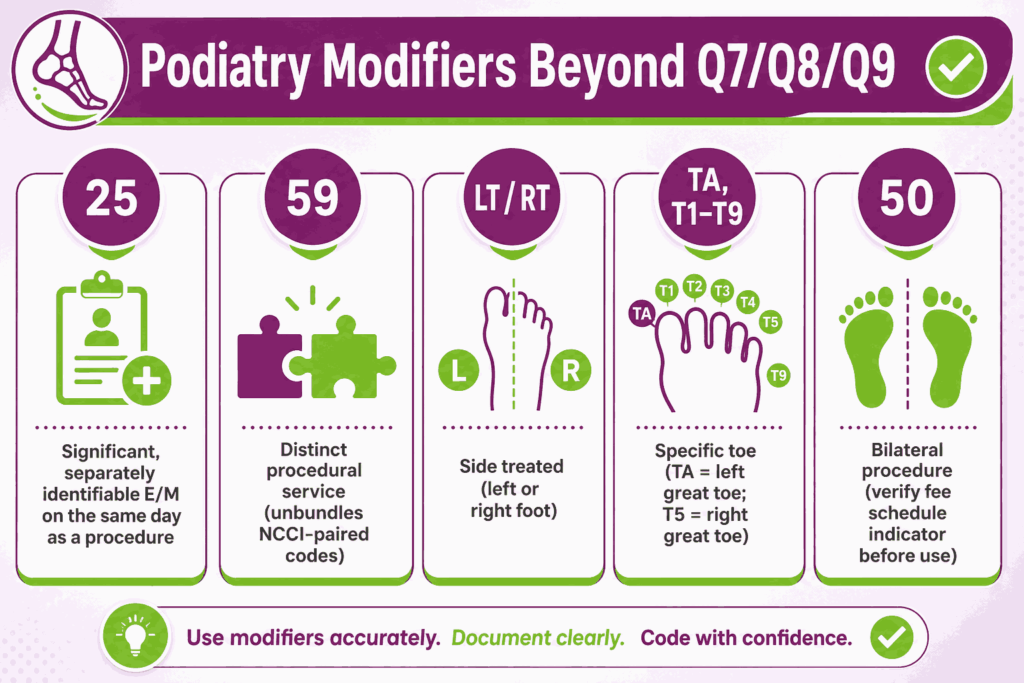
Modifier 50: Bilateral Procedures
Modifier 50 reports a procedure performed on both sides during the same session. Use it only when the CPT code carries a bilateral-eligible indicator on the Medicare Physician Fee Schedule. For most podiatry surgical codes, payers prefer the LT/RT combination over modifier 50; check each payer’s policy before billing. Adding 50 to a code with a bilateral indicator of “0” or “2” triggers a denial.
How Can Effective Denial Management Improve Podiatry Billing?
Denials are inevitable. What separates a healthy podiatry practice from a bleeding one is how fast and how systematically those denials get worked.
What Are the Common Causes of Claim Denials in Podiatry Billing?
Six denial patterns drive most podiatry billing denials. Knowing them by reason code lets you prevent the next one upstream.
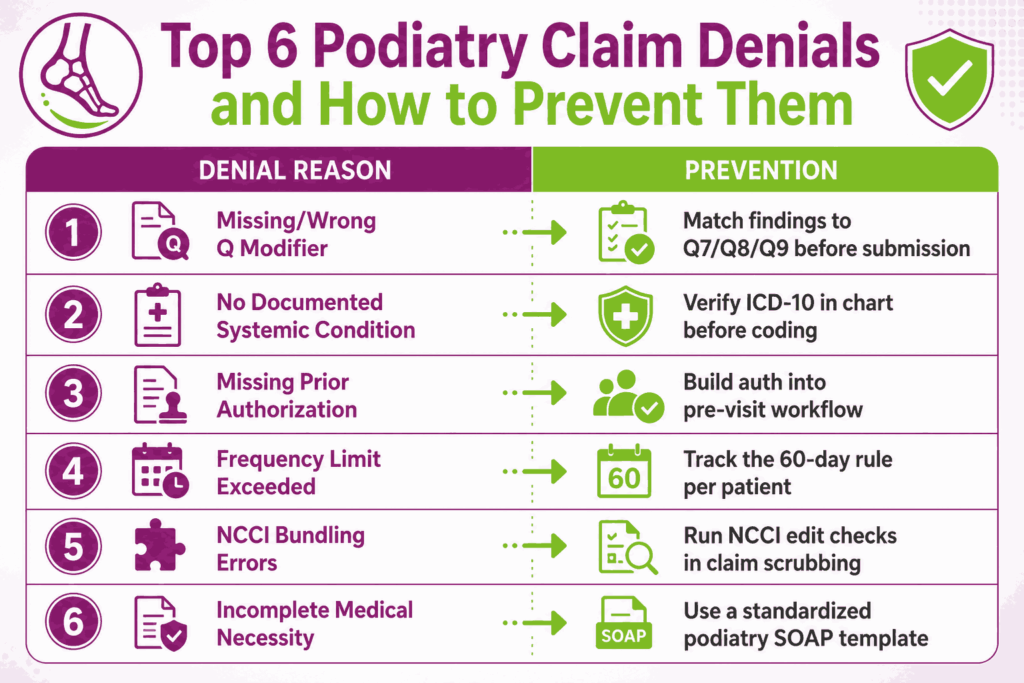
Missing or Incorrect Q Modifier
Routine foot care claims without a Q modifier are denied automatically. The wrong Q modifier, like Q8 when documentation only supports Q9, or Q7 when no Class A finding is recorded, denies just as fast.
No Documented Systemic Condition
Submitting 11720 or 11721 without a qualifying systemic ICD-10 code (diabetes, PVD, peripheral neuropathy) triggers an immediate denial. The diagnosis must be in the medical record, not just on the claim.
Missing Prior Authorization
Custom orthotics, therapeutic shoes, MRI, and elective surgeries usually need prior auth. A claim submitted without it gets denied regardless of medical necessity.
Frequency Limit Exceeded
Routine foot care performed more often than every 60 days gets flagged unless documentation justifies the clinical urgency.
NCCI Edit Violations and Bundling Errors
Pairing mutually exclusive codes (e.g., 11055 with 11305) triggers an NCCI edit. The lower-RVU code drops; sometimes, both deny.
Incomplete Documentation of Medical Necessity
The single largest cause is incomplete documentation. Missing class findings, missing date last seen, vague exam descriptions are a major issue, as all of these read as “no medical necessity” to a payer.
What Strategies Help With Denial Management in Podiatry Billing?
The cheapest denial is the one you never submit.
Pre-Submission Claim Scrubbing
Every claim runs through scrubbing software or a manual checklist before it leaves: NCCI edit check, modifier validation, diagnosis-to-procedure pairing, and demographic verification. Catching errors before submission costs a fraction of appealing them later.
Internal Audits and Coding QA
Run monthly chart audits on a random sample of at least 25 claims per coder. Track findings by code and modifier to surface patterns. A coder repeatedly missing Q9 modifiers is a training issue, not a one-off error.
Continuous Staff Training on Payer Updates
Medicare LCDs and CPT codes change annually. Commercial payer policies shift quarterly. Staff need scheduled time for AAPC updates, MAC bulletins, and payer-specific webinars.
How to Appeal Denied Podiatry Claims
Most denials are appealable. A structured appeal process recovers more revenue than ad-hoc resubmissions. This is especially for medical necessity denials, where supporting documentation can flip the outcome.
Reading the Denial Code and Reason
Start with the Claim Adjustment Reason Code (CARC) and Remittance Advice Remark Code (RARC) on the ERA. CARC 50 (non-covered service), CARC 197 (precertification absent), and CARC 16 (claim lacks information) each take different appeal paths.
Building a Clinical Appeal Package
A strong appeal includes the original claim, the denial letter, the full clinical note for the date of service, documentation of medical necessity (class findings, systemic diagnosis, monofilament results), and a cover letter mapping each piece of evidence to the denial reason.
Peer-to-Peer Review Escalation
When a payer denies for “lack of medical necessity,” request a peer-to-peer review with the payer’s medical director. The provider explains the clinical case directly. Win rates on peer-to-peers run higher than written appeals for medical necessity denials.
KPIs to Track Podiatry Billing Performance
The right metrics tell you whether your podiatry billing process is healthy or quietly bleeding revenue. Top podiatry billing companies review these monthly, not annually.
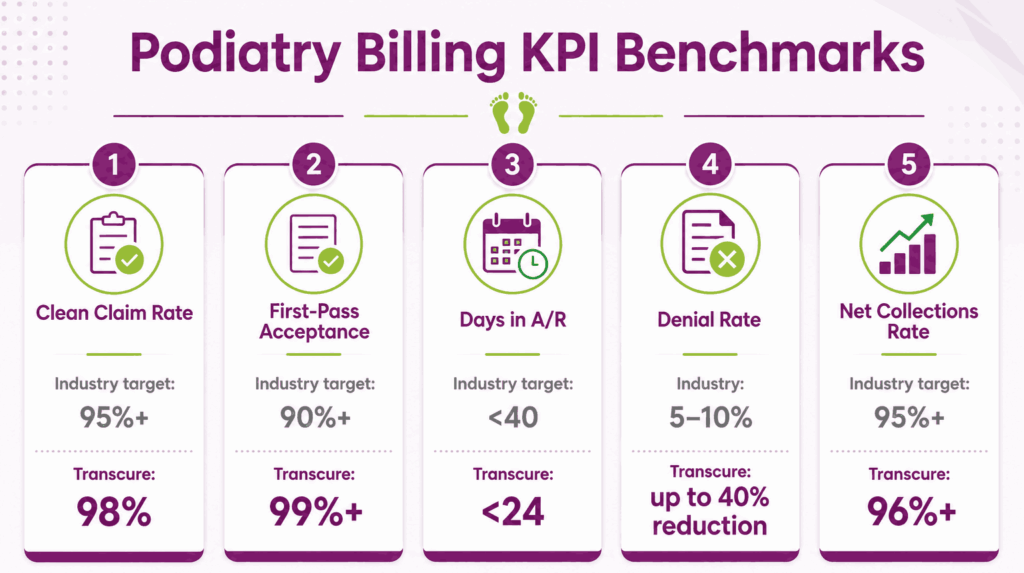
Clean Claim Rate
The percentage of claims that pass scrubbing on the first attempt with no errors. Industry target is 95%+. Transcure clients average a 98% clean claim rate using AI-driven scrubbing.
First-Pass Acceptance Rate
The percentage of claims paid on the first submission without rejection or denial. Below 90% signals upstream problems in coding, eligibility, or documentation. Transcure benchmarks aim for 99%+ first-pass acceptance through AI-powered claim scrubbing.
Days in Accounts Receivable
Average time from claim submission to payment. Industry benchmark is under 40 days, while high performers stay under 30. Transcure targets less than 24 A/R days across podiatry accounts.
Denial Rate by Payer and Reason Code
The percentage of claims denied, segmented by payer and CARC. Industry average runs 5% to 10%. Transcure cuts denial rates by up to 4% through pre-submission scrubbing and Q-modifier QA.
Net Collections Rate
The percentage of contractually allowed revenue actually collected. Healthy podiatry practices target 95%+. Anything under 90% means contractual write-offs or untracked underpayments are eating margin. For example, Transcure promises more than 96% collection rate to its clients.
Frequently Asked Questions About Podiatry Medical Billing
Is Podiatry Billing Covered by Medicare?
Yes, but selectively. Medicare covers podiatry services that treat injuries, diseases, or conditions of the foot, ankle, and lower leg. Routine foot care, like cutting toenails, paring corns and calluses, is excluded unless a qualifying systemic condition is documented with the required class findings.
What Is the Difference Between Routine Foot Care and Medically Necessary Foot Care?
Routine foot care is hygienic maintenance, such as trimming nails, paring corns and calluses, performed on a healthy patient. Medically necessary foot care is the same service performed on a patient with a systemic condition (diabetes, PVD, neuropathy) and documented class findings, which Medicare covers.
When Do You Need a Q Modifier on a Podiatry Claim?
Apply a Q modifier to every routine foot care claim where coverage depends on a systemic condition with class findings. Use Q7 for one Class A finding, Q8 for two Class B findings, and Q9 for one Class B plus two Class C findings.
How Often Can a Patient Receive Nail Debridement Under Medicare?
Once every 60 days. Services performed more frequently can be paid only if the documentation justifies the clinical urgency and the managing physician’s records support it. Claims exceeding the 60-day frequency rule are flagged for medical review.
What Documentation Is Required to Prove Medical Necessity in Podiatry?
A complete SOAP note with the qualifying systemic diagnosis, the specific class findings observed on the same foot being treated, the date last seen by the managing physician (in some MAC jurisdictions), and the clinical reason the service required a podiatrist.
What Are the Most Common Reasons Podiatry Claims Get Denied?
Missing or incorrect Q modifier, no documented systemic condition, missing prior authorization, frequency limit exceeded, NCCI bundling violations, and incomplete medical necessity documentation. Most podiatry billing denials trace back to documentation gaps, not coding mistakes themselves.
How Do You Choose the Best Podiatry Billing Company to Outsource To?
Look for podiatry-specific experience, certified coders, modifier expertise (especially Q7/Q8/Q9), strong KPIs (95%+ clean claim rate, sub-40 days A/R), HIPAA compliance, and transparent reporting. Transcure delivers a 98% clean claim rate with AI-driven scrubbing built for podiatry billing accuracy.






