Orthopedics carries the largest ICD-10 code set of any specialty, and the reason is structural. According to No World Borders, orthopedic conditions span more body regions than any other specialty, with roughly 300 codes covering fractures alone. CMS attributes over one-third of the ICD-10 expansion to laterality, the requirement to mark right, left, or bilateral on each diagnosis.
That specificity is where revenue leaks. A single missing seventh character or an unspecified laterality code can stall a claim or trigger a denial. Insurers read these details closely, and orthopedic billing services exist largely to keep that detail intact across high-volume surgical and clinic encounters.
This guide maps the orthopedic ICD-10 landscape in two layers. The first covers the coding mechanics that govern every diagnosis: chapter structure, laterality, seventh characters, fractures, and aftercare. The second lists the most common conditions by region, with the top codes for each.
What Are Orthopedic ICD-10 Codes?
Orthopedic ICD-10 codes are diagnosis codes that classify musculoskeletal conditions, including joint disease, bone disorders, soft-tissue injuries, and fractures. These codes draw from two ICD-10-CM chapters and feed directly into claim adjudication, medical necessity, and statistical reporting. Orthopedic coding accuracy determines whether a procedure gets reimbursed.
Which ICD-10 Chapters Cover Orthopedic Diagnoses?
Orthopedic diagnoses are split across two ICD-10-CM chapters. Chapter 13 holds chronic and degenerative musculoskeletal conditions. Chapter 19 holds acute injuries.
- Chapter 13 (M00–M99): Diseases of the musculoskeletal system and connective tissue. Covers osteoarthritis, rheumatoid arthritis, osteoporosis, tendon disorders, and back pain.
- Chapter 19 (S00–T88): Injury, poisoning, and certain other consequences of external causes. Covers fractures, dislocations, sprains, and traumatic tendon tears.
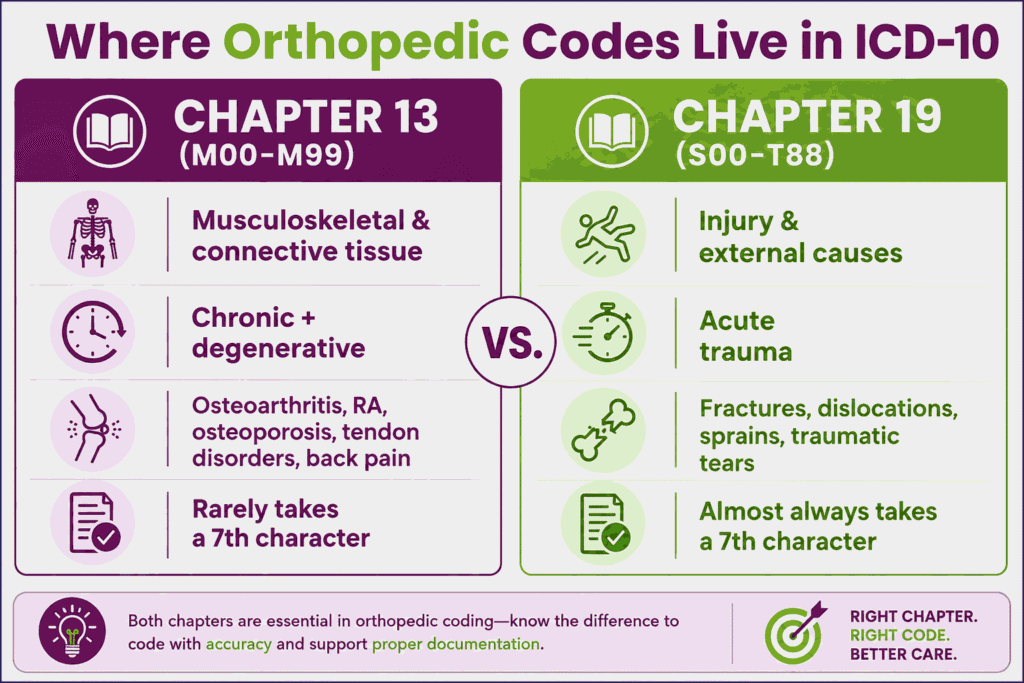
The split matters because the two chapters follow different coding rules. M-codes rarely take a seventh character. S-codes almost always do. A rotator cuff problem coded as degenerative (M75) follows one path; the same tissue coded as traumatic (S43) follows another.
How Is an Orthopedic ICD-10 Code Structured?
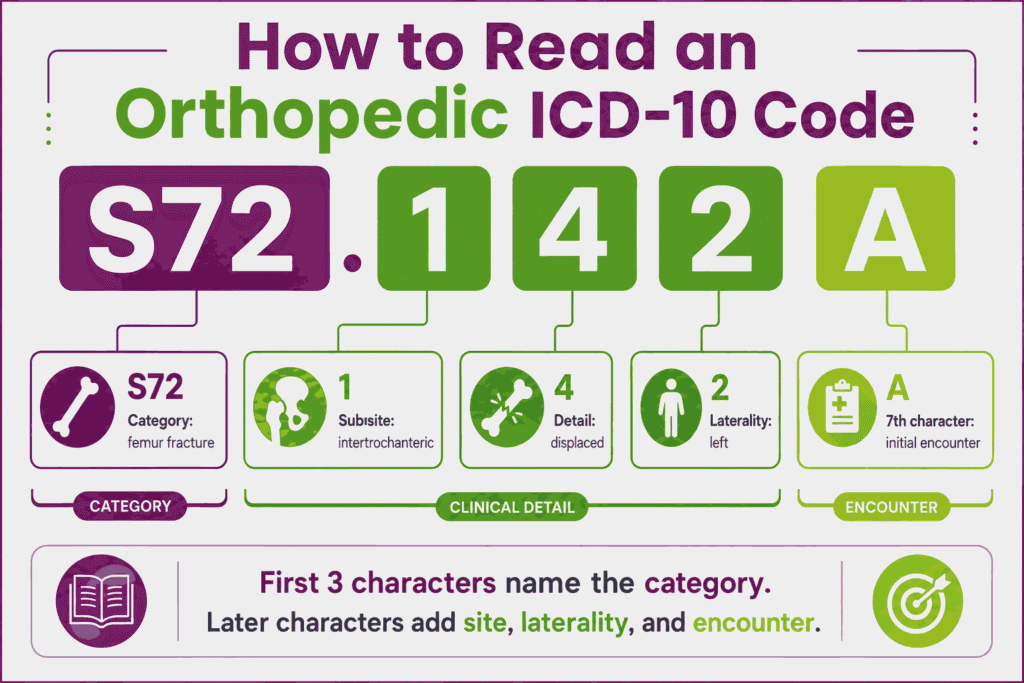
An orthopedic ICD-10 code is an alphanumeric string of three to seven characters, where each position adds clinical detail. The first three characters name the category. Later characters specify site, laterality, and encounter.
Compare a chronic code with an injury code:
- M17.11: Unilateral primary osteoarthritis, right knee. M17 names the category (knee osteoarthritis), the fourth character marks primary type, and the sixth marks the right side.
- S72.142A: Displaced intertrochanteric fracture of the left femur, initial encounter. S72 names femur fracture, middle characters specify location and displacement, and the seventh character A marks the initial encounter.
Codes ending in an unspecified site or unspecified laterality remain billable but invite denials. Specific codes protect reimbursement.
How Do You Code Orthopedic Diagnoses Correctly?
Correct orthopedic coding depends on four documentation elements: laterality, encounter type, fracture detail, and aftercare status. These elements separate a clean claim from a denied one. The condition lists later in this guide supply the codes; this section supplies the rules that make those codes payable.
Why Does Laterality Matter in Orthopedic Coding?
Laterality matters because most orthopedic codes require it, and unspecified laterality is a leading denial trigger. ICD-10 marks each relevant diagnosis as right, left, or bilateral.
Knee osteoarthritis shows the pattern:
- M17.11: Right knee
- M17.12: Left knee
- M17.0: Bilateral
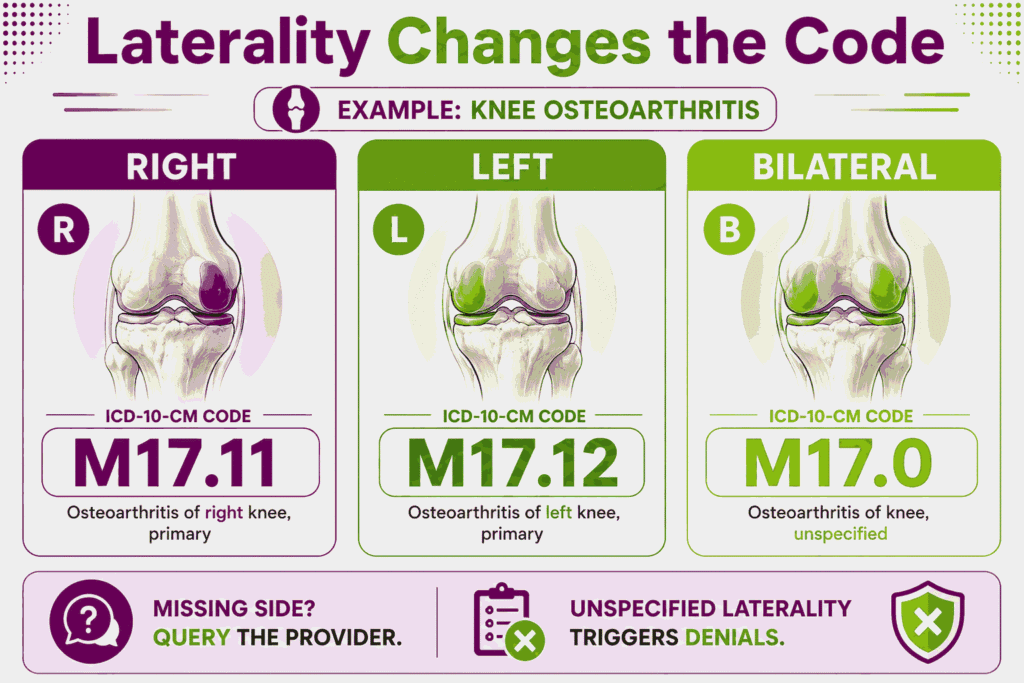
When documentation omits the side, best practice is to query the provider rather than default to an unspecified code. Unspecified laterality confuses payers and weakens medical necessity for site-specific procedures.
What Does the 7th Character Mean?
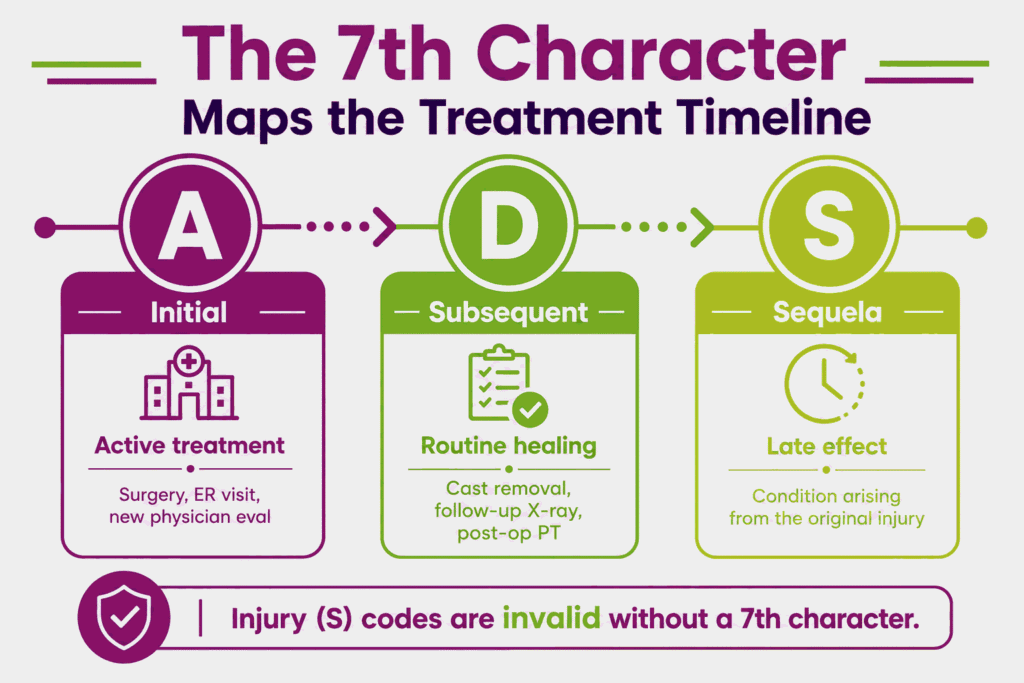
The seventh character marks the episode of care for injury codes, almost all of which begin with S. It identifies where the patient sits in the treatment timeline. Injury codes are invalid without it.
Initial, Subsequent, and Sequela Encounters (A, D, S)
Three seventh characters cover the core episode types:
- A — Initial encounter: Active treatment. Surgery, the emergency visit, or evaluation by a new physician all qualify.
- D — Subsequent encounter: Routine healing care after active treatment. Cast removal, a follow-up X-ray, and post-op physical therapy use D.
- S — Sequela: A condition arising as a direct result of the injury, such as a contracture after a fracture.
Fracture codes expand this set further, adding characters that flag open versus closed and routine versus delayed healing.
Using the X Placeholder
The X placeholder fills empty character positions so the seventh character lands in the seventh slot. Some codes reach only the fifth or sixth character but still require a seventh. The X holds the gap. Staff can reference a detailed ICD 10 codes guide to double-check placeholder formatting before submission. A code that progresses to five characters takes an X in the sixth position, then the encounter character in the seventh. Dropping the placeholder shifts the encounter character into the wrong position and invalidates the code.
How Do You Code Orthopedic Fractures?
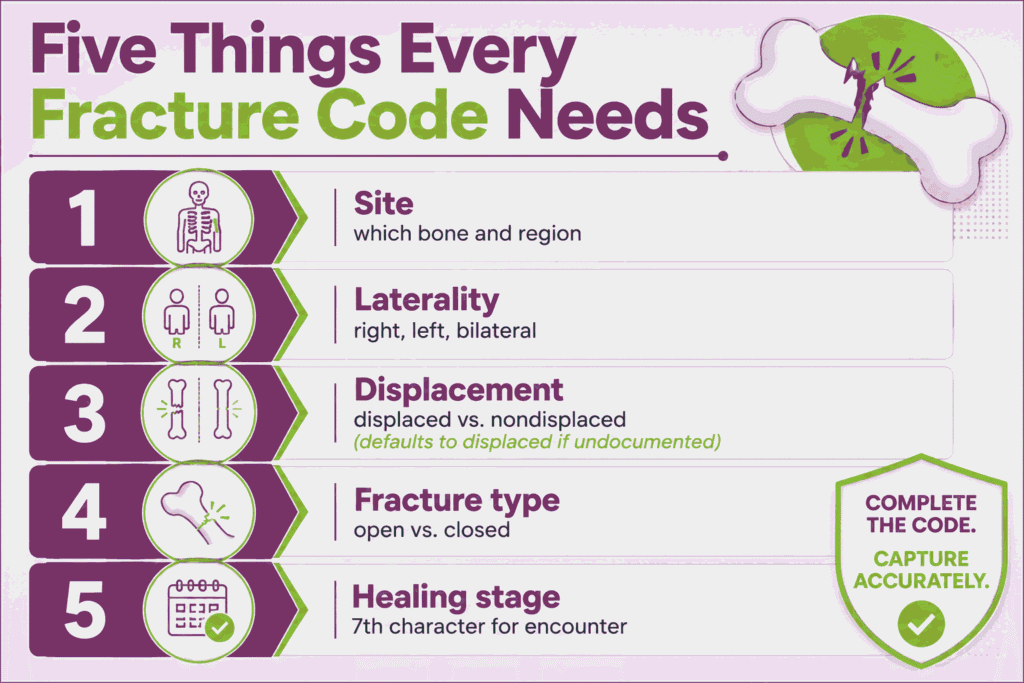
Fracture coding requires five documented elements: site, laterality, displacement, fracture type, and healing stage. Fractures sit in Chapter 19 and represent roughly 300 orthopedic codes. Each element narrows the code.
Displaced vs. Nondisplaced and Open vs. Closed
Displacement and skin integrity define the fracture’s clinical severity. ICD-10 codes default to displaced when documentation is silent, so the distinction must be explicit.
- Displaced: Bone fragments have moved out of alignment.
- Nondisplaced: Fragments remain aligned.
- Closed: Skin over the fracture is intact.
- Open: Bone has broken the skin, raising infection risk.
Open fractures carry a higher coding and reimbursement weight because they demand more intensive management.
Open Fracture Classification and the Gustilo Scale
The Gustilo classification grades open fracture severity and drives the seventh character for many open fracture codes. The scale measures soft-tissue damage and contamination.
ICD-10 maps Gustilo grades to seventh characters for categories such as S52 (forearm) and S82 (lower leg):
- B: Initial encounter, open fracture Type I or II
- C: Initial encounter, open fracture Type IIIA, IIIB, or IIIC
Higher grades signal greater tissue loss and contamination, which support more complex treatment coding.
When Should You Use Orthopedic Aftercare (Z) Codes?
Orthopedic aftercare Z codes apply to surgical follow-up and healing care that is not active treatment, but they never apply to traumatic fracture aftercare. The distinction is a frequent audit target.
Common aftercare codes:
- Z47.89: Encounter for other orthopedic aftercare. Used after surgical procedures during routine recovery.
- Z47.1: Aftercare following joint replacement surgery.
- T84.84: Pain due to internal orthopedic prosthetic device, implant, or graft.
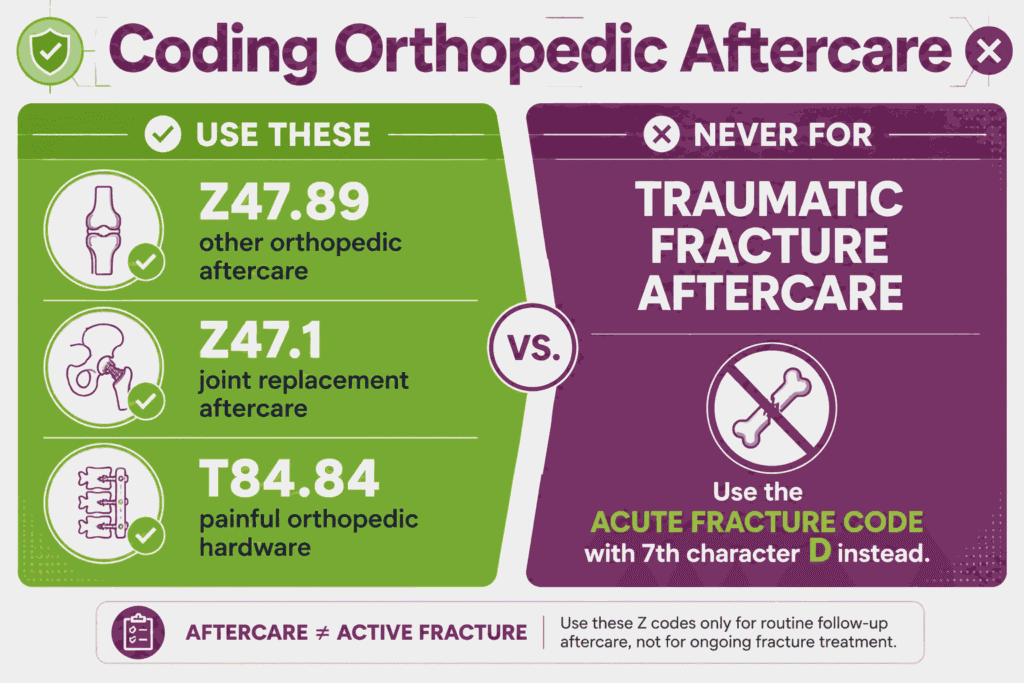
For a healing traumatic fracture, the acute fracture code with a subsequent-encounter seventh character (D) replaces any aftercare Z code. Per the CMS ICD-10-CM Official Guidelines, aftercare Z codes are not used for fracture aftercare. Our complete medical billing guide for orthopedics breaks down these complex sequencing restrictions to keep practice revenue compliant during the post-operative period.
Which ICD-10 Codes Cover the Most Common Orthopedic Conditions?
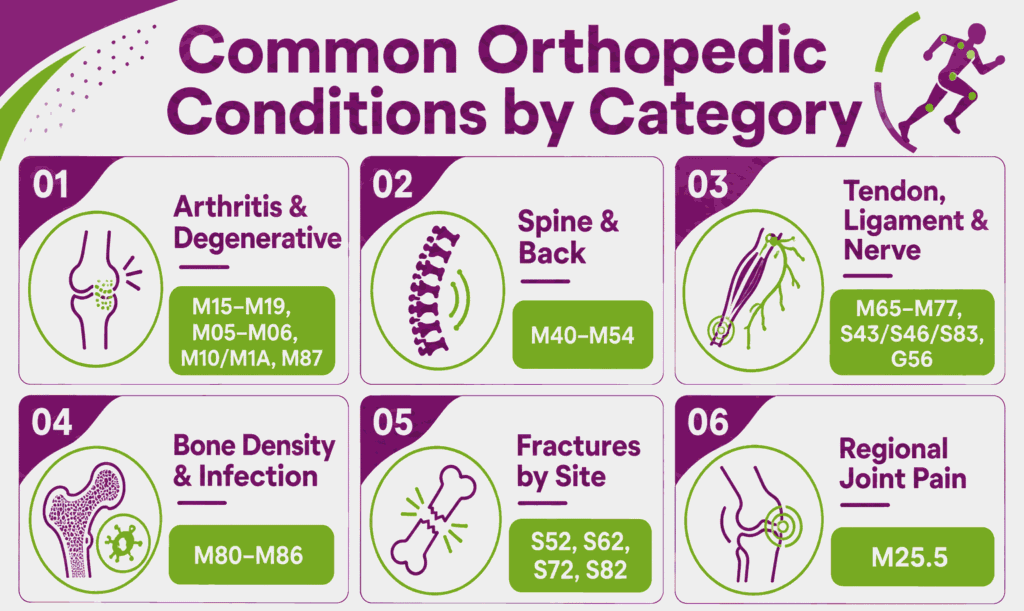
The most common orthopedic conditions cluster into six categories: arthritis and degenerative joint disease, spine disorders, soft-tissue and nerve conditions, bone density and infection, fractures by site, and regional joint pain. Each condition below lists its primary codes. Many conditions carry full code sets across laterality and severity, which the linked guides detail.
Arthritis and Degenerative Joint Codes
Arthritis and degenerative joint conditions sit in Chapter 13 and are coded by joint, laterality, and type. Primary versus secondary classification governs the code path.
Osteoarthritis ICD-10 Codes
Osteoarthritis codes occupy the M15–M19 range and are split by joint and laterality. ICD-10 separates primary, secondary, and post-traumatic osteoarthritis, with the hip and knee carrying the deepest code sets. M17.11 marks right-knee primary osteoarthritis; M16.11 marks the right hip. Generalized osteoarthritis affecting multiple joints uses M15. Full osteoarthritis ICD-10 codes span every major joint with primary and secondary subtypes.
Rheumatoid Arthritis ICD-10 Codes
Rheumatoid arthritis codes fall in the M05–M06 range and distinguish seropositive from seronegative disease. M05 covers rheumatoid arthritis with rheumatoid factor and organ involvement; M06.9 covers unspecified rheumatoid arthritis. Codes specify the affected joint and laterality, and several combine the arthritis with its manifestations. The complete rheumatoid arthritis ICD-10 codes set maps each joint across both serotypes.
Gout ICD-10 Codes
Gout codes sit in the M10 (acute gout) and M1A (chronic gout) categories. Codes specify the cause, such as idiopathic or drug-induced, plus the joint and laterality. M10.9 marks unspecified gout. Chronic gout codes in M1A add a flag for tophus presence. The full gout ICD-10 codes set separates acute flares from chronic tophaceous disease.
Avascular Necrosis ICD-10 Codes
Avascular necrosis codes occupy the M87 category for osteonecrosis. M87.0 covers idiopathic aseptic necrosis of bone; codes specify the bone and laterality. The femoral head is the most common site. Drug-induced and post-traumatic osteonecrosis carry separate subcategories. The avascular necrosis ICD-10 codes set details each site and cause.
Spine and Back Codes
Spine and back codes draw mostly from the M40–M54 range and code by spinal region. Region specificity, cervical through sacral, separates most codes.
Back Pain ICD-10 Codes
Back pain codes center on M54 (dorsalgia) and specify spinal region. M54.5 was replaced by more specific low back pain codes, including M54.50 (unspecified), M54.51 (vertebrogenic), and M54.59 (other). M54.6 covers thoracic spine pain. The full back pain ICD-10 codes set maps each spinal level.
Sciatica ICD-10 Codes
Sciatica codes sit in the M54.3 subcategory and require laterality. M54.31 marks right-side sciatica; M54.32 marks the left. M54.4 covers lumbago with sciatica, again split by side. The complete sciatica ICD-10 codes set separates pure sciatica from combined lumbago presentations.
Herniated Disc ICD-10 Codes
Herniated disc codes fall in the M50 (cervical) and M51 (thoracic and lumbar) categories. Codes specify the region and whether myelopathy or radiculopathy is present. M51.26 covers lumbar disc displacement; M50.20 covers cervical disc displacement. The herniated disc ICD-10 codes set details each region and neurological involvement.
Spinal Stenosis ICD-10 Codes
Spinal stenosis codes occupy the M48.0 subcategory and specify region. M48.06 marks lumbar spinal stenosis; M48.02 marks the cervical region. Codes further distinguish stenosis with and without neurogenic claudication. The full spinal stenosis ICD-10 codes set maps each spinal level.
Scoliosis ICD-10 Codes
Scoliosis codes sit in the M41 category and specify type and region. M41.9 covers unspecified scoliosis; idiopathic, neuromuscular, and degenerative subtypes carry distinct codes. Adolescent idiopathic scoliosis uses the M41.1 subcategory. The complete scoliosis ICD-10 codes set details each curve type and spinal region.
Tendon, Ligament, and Nerve Codes
Tendon, ligament, and nerve codes span both chapters, splitting by chronic (M-codes) versus traumatic (S-codes) origin. Documentation of cause determines the chapter.
Rotator Cuff Tear ICD-10 Codes
Rotator cuff tear codes split by cause. Non-traumatic tears use M75.1 with laterality and tear severity; traumatic tears use S46.01. M75.121 marks a complete, non-traumatic tear of the right shoulder, and M75.111 marks an incomplete tear. The distinction drives both the seventh-character requirement and audit risk. The full rotator cuff tear ICD-10 codes set separates degenerative from traumatic tears across partial and complete severity.
ACL Tear ICD-10 Codes
ACL tear codes sit in the S83.51 subcategory as traumatic injuries requiring a seventh character. S83.511A marks a right ACL sprain, initial encounter. Codes specify laterality and encounter type. The complete ACL tear ICD-10 codes set details each side across the encounter timeline.
Meniscus Tear ICD-10 Codes
Meniscus tear codes split by cause and location. Acute tears use S83.2 with laterality and encounter; degenerative tears use M23. S83.241A marks a right medial meniscus tear, initial encounter. The meniscus tear ICD-10 codes set separates acute injuries from chronic degeneration.
Frozen Shoulder ICD-10 Codes
Frozen shoulder codes occupy the M75.0 subcategory for adhesive capsulitis. M75.01 marks the right shoulder; M75.02 marks the left. The condition codes by laterality only. The full frozen shoulder ICD-10 codes set details each side.
Bursitis ICD-10 Codes
Bursitis codes span the M70–M71 range and specify joint and laterality. M70.5 covers knee bursitis; M75.5 covers shoulder bursitis. Codes distinguish occupational and infective causes. The complete bursitis ICD-10 codes set maps each joint.
Tendonitis ICD-10 Codes
Tendonitis codes fall across the M65–M77 range by site. M65 covers synovitis and tenosynovitis; M76 and M77 cover lower- and upper-limb enthesopathies. M77.0 marks medial epicondylitis. The tendonitis ICD-10 codes set details each tendon site.
Plantar Fasciitis ICD-10 Codes
Plantar fasciitis codes use M72.2, a single code without laterality. M72.2 covers plantar fascial fibromatosis. The condition codes simply, though related heel conditions carry separate codes. The plantar fasciitis ICD-10 codes set covers the condition and its differentials.
Carpal Tunnel Syndrome ICD-10 Codes
Carpal tunnel syndrome codes sit in the G56.0 subcategory and require laterality. G56.01 marks right-side carpal tunnel; G56.02 marks the left. The code originates in Chapter 6 (nervous system), not the musculoskeletal chapter. The full carpal tunnel syndrome ICD-10 codes set details each side.
Bone Density and Infection Codes
Bone density and infection codes draw from the M80–M86 range and code by cause and fracture status. Pathological fracture presence changes the code.
Osteoporosis ICD-10 Codes
Osteoporosis codes split by fracture status. M81 covers osteoporosis without current pathological fracture; M80 covers osteoporosis with current pathological fracture and requires a seventh character. M81.0 marks age-related osteoporosis. The complete osteoporosis ICD-10 codes set separates uncomplicated disease from fracture presentations.
Osteomyelitis ICD-10 Codes
Osteomyelitis codes occupy the M86 category and specify acute versus chronic and the affected bone. M86.0 covers acute hematogenous osteomyelitis; M86.6 covers chronic osteomyelitis. Codes specify site and laterality. The full osteomyelitis ICD-10 codes set details each bone across acute and chronic forms.
Fracture and Acute Injury Codes by Site
Fracture and acute injury codes sit in Chapter 19 and require the full five-element documentation set. Each code carries a seventh character for encounter type.
Hip Fracture ICD-10 Codes
Hip fracture codes fall in the S72 category for femur fractures. S72.0 covers femoral neck fractures; S72.1 covers intertrochanteric fractures. S72.142A marks a displaced left intertrochanteric fracture, initial encounter. Over 300,000 hip fractures occur annually in the United States. The complete hip fracture ICD-10 codes set maps each location across laterality and encounter.
Ankle Fracture ICD-10 Codes
Ankle fracture codes occupy the S82 category and specify the malleolus and laterality. S82.5 covers medial malleolus fractures; S82.6 covers lateral malleolus fractures. Each requires displacement detail and a seventh character. The full ankle fracture ICD-10 codes set details each fracture site.
Wrist Fracture ICD-10 Codes
Wrist fracture codes are split between the radius (S52) and carpal bones (S62). S52.5 covers distal radius fractures, the most common wrist fracture; S62.0 covers scaphoid fractures. Codes require laterality, displacement, and encounter. The complete wrist fracture ICD-10 codes set details each bone.
Compartment Syndrome ICD-10 Codes
Compartment syndrome codes sit in the T79.A category for traumatic compartment syndrome. T79.A1 covers upper-extremity compartment syndrome; T79.A2 covers the lower extremity. Non-traumatic compartment syndrome uses M79.A. The full compartment syndrome ICD-10 codes set separates traumatic from non-traumatic forms.
Joint and Regional Pain Codes
Joint and regional pain codes use the M25.5 subcategory when no specific diagnosis applies. These codes capture symptoms pending a definitive diagnosis.
Knee Pain ICD-10 Codes
Knee pain codes use M25.56 with laterality. M25.561 marks right knee pain; M25.562 marks the left. These codes apply when no structural diagnosis is established. The full knee pain ICD-10 codes set details each side and related symptom codes.
Shoulder Pain ICD-10 Codes
Shoulder pain codes use M25.51 with laterality. M25.511 marks right shoulder pain; M25.512 marks the left. The codes serve as symptom codes pending diagnosis. The complete shoulder pain ICD-10 codes set details each side.
Why Do Orthopedic Claims Get Denied?
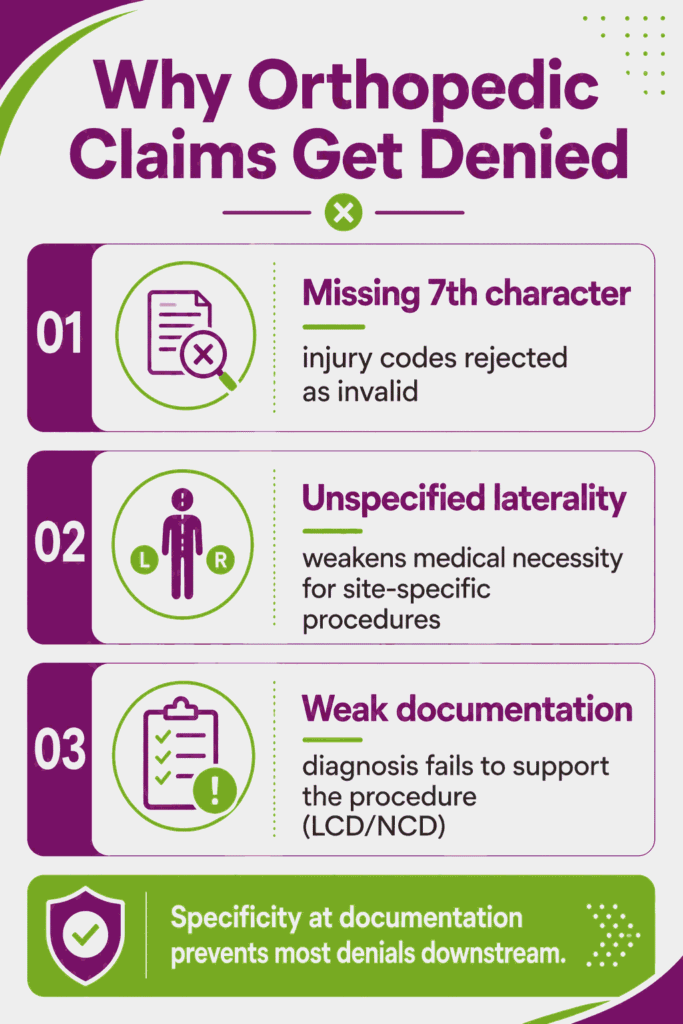
Orthopedic claims get denied primarily from missing seventh characters, unspecified laterality, and weak documentation of medical necessity. Orthopedic coding carries more variables than most specialties, so each variable becomes a denial point. Specificity at the documentation stage prevents most denials downstream. Specialized orthopedic billing services prevent these administrative breakdowns by scrubbing claims for compliance prior to clearinghouse transmission.
What Documentation Supports Orthopedic Code Selection?
Orthopedic code selection requires documentation of laterality, displacement, encounter phase, and radiographic findings. The medical record must state which side, the fracture or lesion type, and the treatment stage. Radiographic findings support code selection objectively. Local and national coverage determinations (LCD and NCD) define which diagnoses justify which procedures. When the diagnosis fails to support the procedure, the claim falls on medical necessity.
How Do You Reduce Orthopedic Coding Denials?
Reducing orthopedic coding denials requires three practices: coding to full specificity, catching missing seventh characters before submission, and scrubbing claims at the front end. Unspecified codes raise audit flags and slow reimbursement. Software glitches sometimes drop seventh characters automatically, so pre-submission review catches the error. Experienced billing companies for orthopedic practices handle this end-to-end reconciliation loop seamlessly, alongside eligibility verification and prior authorization for elective procedures.
Orthopedic ICD-10 Coding FAQs
What Is the Most Common Orthopedic ICD-10 Code?
The most common orthopedic ICD-10 codes vary by practice, but low back pain (M54.50), knee osteoarthritis (M17 series), and unspecified fracture codes rank among the highest-volume diagnoses. Pain and scoliosis codes also appear frequently in clinic settings.
Is There One ICD-10 Code for Orthopedic Pain?
No single ICD-10 code covers all orthopedic pain. Regional pain codes in the M25.5 subcategory cover joint pain by site, while M79 codes cover broader musculoskeletal and soft-tissue pain. The code matches the documented location.
What ICD-10 Code Is Used After Orthopedic Surgery?
Z47.89 (encounter for other orthopedic aftercare) and Z47.1 (aftercare following joint replacement) cover routine post-surgical recovery. Traumatic fracture aftercare uses the acute fracture code with a subsequent-encounter seventh character instead of a Z code.
How Often Do Orthopedic ICD-10 Codes Change?
Orthopedic ICD-10 codes update annually on October 1, when CMS releases the new fiscal-year code set. Updates add, revise, and retire codes, so coding references require yearly review.