2026 Coding and Billing Guide")
Gastroesophageal reflux disease without esophagitis is coded as ICD-10-CM K21.9. The code applies when stomach acid refluxes into the esophagus without inflammation or mucosal damage. It represents the least severe stage of the disease.
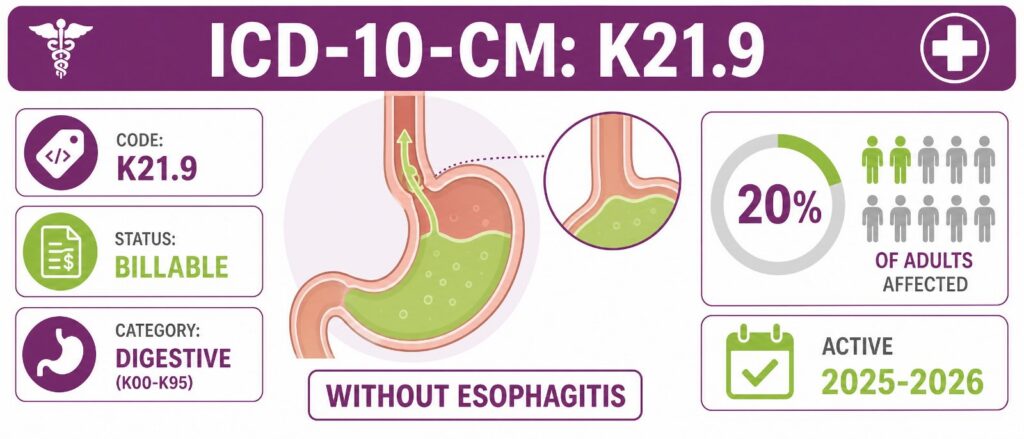
K21.9 sits in the K20-K31 range, covering diseases of the esophagus, stomach, and duodenum. The 2026 edition became effective on October 1, 2025. It is a billable, specific code valid for HIPAA-covered transactions through September 30, 2026.
GERD is one of the most common GI diagnoses, which makes K21.9 a high-volume code. High volume means high financial exposure. A single recurring documentation gap can multiply into hundreds of denied claims across a practice.
This guide covers the clinical basis of K21.9, its symptoms, the full K21 family, documentation standards, CPT pairings, modifier and medical necessity rules, sequencing, denial patterns, and the questions coders ask most.
What Is the ICD-10 Code for GERD Without Esophagitis?
The ICD-10-CM code for GERD without esophagitis is K21.9. It denotes cases of gastroesophageal reflux disease where there is no evidence of esophagitis. Reflux occurs, but the esophageal lining shows no inflammation or erosion.
Quick reference facts for K21.9:
- Code: K21.9
- Description: Gastro-esophageal reflux disease without esophagitis
- Category: Diseases of the digestive system (K00-K95)
- Status: Billable and specific, no further sub-classification
- Validity: Active October 1, 2025, through September 30, 2026
- MS-DRG: Grouped within MS-DRG 391, digestive disorders with MCC
GERD affects roughly 20% of adults in the United States, and K21.9 is the most common form reported. The code has been in use since ICD-10 was implemented in 2015. The defining phrase is “without esophagitis.”
What Does K21.9 Mean Clinically?
K21.9 captures GERD driven by a weak lower esophageal sphincter. The lower esophageal sphincter normally prevents backflow, and when it weakens or relaxes inappropriately, stomach acid enters the esophagus. No tissue damage is present at this stage.
Stomach acid is highly corrosive. It is made primarily of hydrochloric acid, along with enzymes, mucus, and electrolytes. Repeated exposure irritates the esophageal lining, yet K21.9 applies only while that lining stays free of inflammation.
The disease is chronic by nature. Left untreated, it can progress to esophagitis, strictures, or Barrett’s esophagus over time. K21.9 marks the entry point of that spectrum, before structural change appears.
What Is the Difference Between Acute and Chronic GERD?
The code does not separate new-onset from long-standing GERD. K21.9 does not distinguish between acute and chronic presentations, though documenting symptom duration still supports clinical decision-making.
A practical framework helps the chart tell a complete story:
- Acute GERD: symptoms present for less than three months
- Chronic GERD: persistent symptoms beyond three months
- Coding impact: neither label changes the code, but both justify the service level billed
Duration notes strengthen medical necessity even when the code stays fixed. The clinical picture, not the code, carries that weight.
What Symptoms Are Linked to K21.9?
GERD presents through typical and atypical symptoms. Coders should recognize both, since atypical cases still map to K21.9 when esophagitis is absent. The symptom set also justifies the diagnostic workup billed alongside the code.
Typical symptoms include:
- Heartburn, a burning sensation in the chest
- Acid regurgitation into the throat or mouth
- A sour or bitter taste after meals
- Chest discomfort, often after eating or when lying down
Atypical and extraesophageal symptoms include:
- Chronic dry cough without a respiratory cause
- Asthma-like symptoms or wheezing
- Difficulty swallowing
- Laryngopharyngeal reflux reaching the upper airway
Laryngopharyngeal reflux is an extraesophageal manifestation of gastroesophageal reflux affecting the upper aerodigestive tract. Atypical patients rarely show endoscopic esophagitis, so pH monitoring often confirms the diagnosis before K21.9 is assigned.
How Does K21.9 Differ From Other K21 Codes?
The K21 category splits by the presence of esophagitis and bleeding. CMS implemented refined GERD coding distinctions effective October 1, 2024. Selecting the wrong member of the family triggers denials and audit flags.
| Code | Description | When To Use |
|---|---|---|
| K21.00 | GERD with esophagitis, without bleeding | Endoscopy confirms inflammation, no bleeding |
| K21.01 | GERD with esophagitis, with bleeding | Esophagitis documented with active bleeding |
| K21.8 | GERD with other esophageal manifestations | Less common or unspecified esophageal issues |
| K21.9 | GERD without esophagitis | No inflammation or mucosal injury found |
When documentation states GERD is associated with esophagitis, K21.00 or K21.01 applies instead of K21.9. Select K21.8 when GERD produces less common esophageal issues or coexists with esophageal motility disorders.
The presence of esophagitis is the dividing line. For practices coding across the full digestive panel, our reference on Gastroenterology CPT Codes maps the procedure codes that attach to each diagnosis, while our broader index of gastroenterology ICD-10 codes provides full diagnostic cross-references.
When Should You Assign K21.9?
Assign K21.9 when the provider documents GERD and the record confirms no esophagitis. Use it when the diagnosis rests on findings from endoscopic or other diagnostic evaluations. The assessment portion of the note should name the condition directly.
Use K21.9 in these situations:
- The provider documents GERD or GERD without esophagitis in the assessment
- Endoscopy results show no esophageal inflammation or erosion
- Reflux symptoms appear without confirmed mucosal injury
- The diagnosis is confirmed, not suspected, in the outpatient setting
Avoid K21.9 if the notes mention esophagitis, bleeding, or anatomical abnormalities such as a hernia. In those cases, assign the more specific code that reflects the documented severity.
What If Only Symptoms Are Documented?
Do not default to K21.9 when only a symptom appears. If heartburn alone is documented, report R12 rather than K21.9. Symptom codes like R12 can supplement a confirmed GERD diagnosis, but they do not replace it. The symptom code reflects the record accurately and survives audit review.
How Do Inpatient and Outpatient Rules Differ?
Coding GERD shifts based on the care setting. The ICD-10-CM Official Guidelines treat unconfirmed diagnoses differently in each. Knowing the split prevents coding a suspected condition as confirmed.
| Setting | Rule for Unconfirmed GERD | Action |
|---|---|---|
| Inpatient | Suspected or differential GERD may be coded as confirmed | Assign K21.9 if documented as probable |
| Outpatient | Suspected or rule-out statements cannot be coded as confirmed | Report symptoms until diagnosis is confirmed |
In the outpatient setting, suspected, rule-out, or differential statements are not confirmed diagnoses and cannot be assigned. Coders report the patient’s symptoms instead until the provider confirms GERD.
One Excludes 1 note also applies. Newborn esophageal reflux is coded separately as P78.83 and should not be reported with K21. No other chapter-specific notes apply to GERD beyond these guidelines.
What Documentation Supports K21.9?
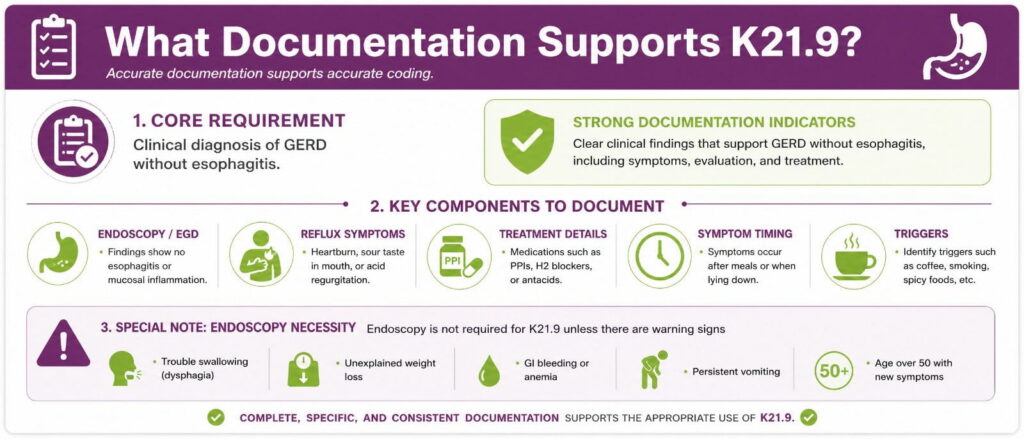
Patients expect the record to confirm both the diagnosis and the absence of esophagitis. The provider note must state GERD without esophagitis, and endoscopy should confirm no inflammation when performed. Weak documentation is the leading driver of K21.9 denials.
Strong documentation for K21.9 includes:
- A clinical diagnosis stating GERD in the provider assessment
- Endoscopy or EGD findings showing no esophageal inflammation
- Reflux symptoms such as heartburn, regurgitation, or sour taste
- Treatment details, including PPIs, H2 blockers, or antacids
- Symptom timing, such as after meals or when lying down
- Triggers like coffee, alcohol, or smoking that raise stomach acid
Endoscopy is not always required, since symptom response to PPIs can support a first diagnosis. Warning signs such as trouble swallowing, weight loss, or bleeding do make endoscopy necessary.
What Does a Clean Note Look Like?
A strong note links the diagnosis to the test results plainly. A model example reads: patient reports heartburn and regurgitation, EGD shows no esophagitis, pH monitoring confirms reflux, assessment is GERD without esophagitis, PPI prescribed.
The weak version states only “GERD” with no mention of esophagitis status. Clinical documentation improvement closes that gap. Coder queries and provider education keep the esophagitis status explicit on every reflux encounter.
Which CPT Codes Pair With K21.9?
GERD claims rarely stand on the diagnosis code alone. K21.9 attaches to evaluation and procedure codes that establish medical necessity. Matching the right CPT code to the encounter protects reimbursement.
| CPT Code | Procedure | Typical Use With K21.9 |
|---|---|---|
| 99202-99215 | Office or outpatient E/M visit | Initial and follow-up reflux evaluation |
| 43235 | Upper GI endoscopy, diagnostic | Rule out esophagitis and mucosal damage |
| 43239 | Upper GI endoscopy with biopsy | Tissue sampling when findings are unclear |
| 91010 | Esophageal motility study | Assess sphincter and esophageal function |
| 91034 | Esophageal pH monitoring | Confirm acid reflux frequency |
| 43280 | Laparoscopic fundoplication | Surgical repair for refractory GERD |
Common pairings include EGD, esophageal pH monitoring, and surgical fundoplication when GERD does not respond to medication. Each procedure must connect logically to the documented reflux workup.
A diagnostic EGD billed with K21.9 confirms the absence of esophagitis and supports the code. Mismatched pairings invite payer scrutiny. Practices managing high GI claim volume often outsource this logic to specialized gastroenterology billing services built around endoscopy workflows.
How Do Modifiers and Medical Necessity Apply?
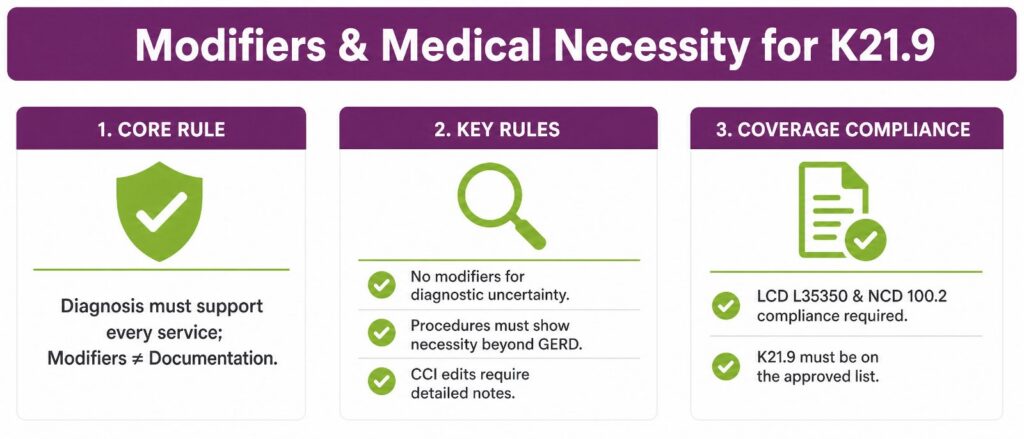
K21.9 carries specific compliance demands when paired with procedures. The diagnosis must support each service on the claim. Modifiers cannot substitute for documentation.
Key medical necessity rules for K21.9:
- Outpatient claims should not use modifiers that hint at diagnostic uncertainty.
- Procedures such as endoscopy must show medical necessity beyond basic GERD management.
- Modifiers cannot bypass Correct Coding Initiative edits, and each code pair needs detailed documentation.
Coverage policy adds another layer. Local Coverage Determination L35350 and National Coverage Determination 100.2 require K21.9 to appear on the approved diagnosis list for the procedure performed. Linking K21.9 to a procedure is not enough, since the diagnosis must be clinically present and documented.
Coverage for any service depends on payer policy and documentation strength. K21.9 is a recognized billable code, but the chart behind it determines payment.
What Codes Relate To or Exclude K21.9?
Several codes sit near K21.9 and require careful separation. Coding the adjacent condition by mistake distorts the record and reimbursement. Knowing the neighbors prevents both errors.
| Code | Condition | Relationship To K21.9 |
|---|---|---|
| R12 | Heartburn | Use when only the symptom is documented |
| K44.9 | Hiatal hernia | May coexist with GERD; sequence separately |
| K21.00 | GERD with esophagitis, no bleeding | Use when inflammation is confirmed |
| K22.70 | Barrett’s esophagus without dysplasia | Use when GERD progresses to Barrett’s |
| P78.83 | Newborn esophageal reflux | Excludes 1, never report with K21 |
A linked condition, such as a hiatal hernia, may require an additional code alongside the GERD diagnosis. GERD can also act as the underlying cause of Barrett’s esophagitis, where abnormal cells replace the normal lining and can progress toward cancer.
One differential deserves attention. Some patients who appear to have GERD actually have eosinophilic esophagitis, a separate disease where white blood cells build up in the esophagus. Endoscopy and biopsy distinguish the two.
How Should You Sequence K21.9 With Other Conditions?
Sequencing matters when GERD coexists with another condition. The underlying cause usually leads. GERD then follows as a secondary diagnosis.
The most common sequencing scenario involves a hiatal hernia:
- Identify the primary condition. When GERD is secondary to a diaphragmatic hernia, code the hernia first.
- List GERD second. Use K44 as the primary code and K21.9 as a secondary diagnosis when GERD is also documented.
- Add complication codes. If GERD leads to ulcers, bleeding, or anemia, add codes to capture the full clinical picture.
Correct sequencing supports accurate severity classification. It also protects reimbursement when payers review the diagnosis order on complex claims.
Why Do K21.9 Claims Get Denied?
K21.9 denials usually trace back to documentation gaps rather than the code itself. Unspecified or incorrect coding causes claim rejections, improper reimbursement, and payer audit exposure. A growing accounts receivable backlog often follows. To address these systemic leakage patterns, referencing an operational gastroenterology billing guide can help back-office teams audit clinical records for prerequisite documentation before claims are filed.
The most frequent K21.9 denial causes are:
- Missing confirmation: the record never states that esophagitis is absent
- Symptom coding error: K21.9 used when only heartburn was documented
- Wrong family member: esophagitis present, but K21.9 assigned anyway
- No medical necessity: the procedure lacks a supporting diagnosis link
- Unconfirmed diagnosis: a rule-out statement coded as confirmed in the outpatient
- Sequencing error: GERD coded first when a hernia is the primary cause
Coding GERD without confirming the absence of esophagitis creates documentation errors, coding pitfalls, and audit risk together. The single most common mistake is using K21.9 interchangeably with the esophagitis codes without checking the record.
Denial recovery drains staff hours that revenue teams cannot spare. Transcure handles gastroenterology billing end-to-end, from coding accuracy to denial prevention.
How Do You Bill K21.9 Correctly?
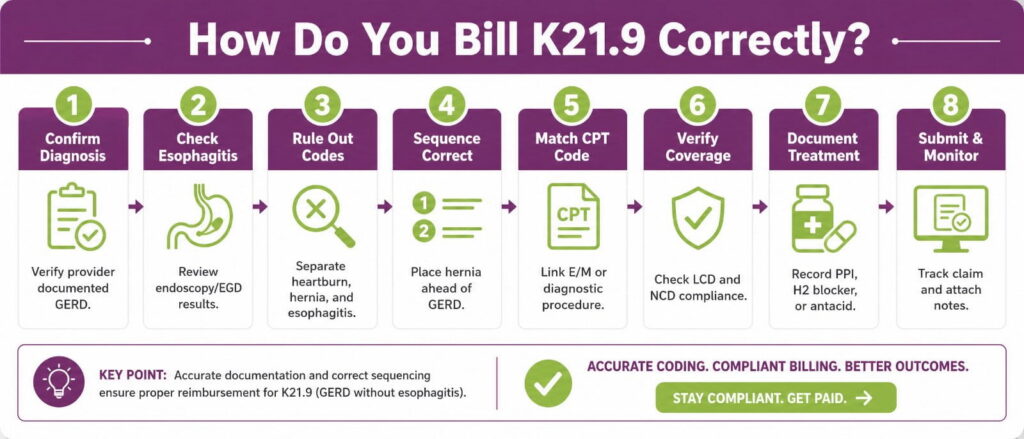
Billing K21.9 cleanly follows a repeatable sequence. Each step closes a common gap that payers exploit to deny claims. Work them in order on every reflux encounter.
- Confirm the diagnosis. Verify the provider documented GERD in the assessment, not just symptoms.
- Check for esophagitis. Review endoscopy or EGD results to confirm no inflammation is present.
- Rule out related codes. Separate heartburn, hiatal hernia, and esophagitis codes before assigning K21.9.
- Sequence correctly. Place any underlying condition, such as a hernia, ahead of the GERD code.
- Match the CPT code. Link the E/M or diagnostic procedure that supports medical necessity.
- Verify coverage. Confirm K21.9 appears on the approved diagnosis list for LCD and NCD compliance.
- Document treatment. Record PPI, H2 blocker, or antacid therapy tied to the diagnosis.
- Submit and monitor. Track the claim and attach the supporting note to any denial.
Following this sequence keeps K21.9 claims compliant and reduces rework. Accuracy at the coding stage costs far less than appeals at the back end.
Frequently Asked Questions
Is K21.9 a billable code?
Yes. K21.9 is a billable, specific ICD-10-CM code valid through September 30, 2026. It groups to MS-DRG 391 and needs no decimal extension for reimbursement.
What is the difference between K21.9 and K21.00?
K21.9 reports GERD without esophagitis. K21.00 requires endoscopy confirming inflammation without bleeding, while K21.01 adds active bleeding. Documented esophagitis status drives the entire choice.
Can I use K21.9 for acid reflux?
Yes. Acid reflux and GERD share the code when no esophageal damage exists. GERD is diagnosed when symptoms occur more than twice weekly. Use K21.00 if esophagitis appears.
Does K21.9 require endoscopy?
Not always. Symptoms and PPI response can support a first diagnosis. Warning signs like dysphagia, weight loss, or bleeding require endoscopy. pH monitoring confirms atypical reflux cases.
How do I code GERD with a hiatal hernia?
Code the hernia first. Use K44 as primary and K21.9 as secondary when GERD is documented. Add complication codes if ulcers, bleeding, or anemia develop alongside reflux.
Can R12 and K21.9 appear on the same claim?
Yes, when supported. R12 can supplement a confirmed K21.9 diagnosis but cannot replace it. In outpatient settings, report symptoms alone until the provider confirms GERD.